También podría gustarte
- CBD. El cannabis medicinal: Guía para el pacienteDe EverandCBD. El cannabis medicinal: Guía para el pacienteCalificación: 5 de 5 estrellas5/5 (7)
- Metodología de la Investigación ClínicaDe EverandMetodología de la Investigación ClínicaCalificación: 4 de 5 estrellas4/5 (1)
- Reanimacion de Control de DañosDocumento29 páginasReanimacion de Control de DañosDayana Florez palacioAún no hay calificaciones
- Radiología de La EmergenciaDocumento93 páginasRadiología de La EmergenciaSociedad Científica de Estudiantes de Medicina de Ica50% (6)
- Sindrome de CrouzonDocumento18 páginasSindrome de CrouzonCaleb Quispe Medina100% (2)
- COLANGIORMDocumento21 páginasCOLANGIORMHelber MHAún no hay calificaciones
- Monitoreo Paciente NeurointensivoDocumento59 páginasMonitoreo Paciente Neurointensivodoriszan100% (4)
- CacuDocumento21 páginasCacuManfred PalomequeAún no hay calificaciones
- ICTERICIADocumento21 páginasICTERICIAFabiola López GarcíaAún no hay calificaciones
- Prealta Danna CarolinaDocumento2 páginasPrealta Danna CarolinaPediatria HGZ11Aún no hay calificaciones
- Protocolos MedicosDocumento10 páginasProtocolos MedicosAbel Acebo FernandezAún no hay calificaciones
- Clase 03a Uci 2018 - I Monitoreo Del Paciente Critico AbrDocumento52 páginasClase 03a Uci 2018 - I Monitoreo Del Paciente Critico AbrWilanderson Correa100% (2)
- Examen Parcial - Semana 4 - Higiene IV CecyDocumento14 páginasExamen Parcial - Semana 4 - Higiene IV CecyMarioAún no hay calificaciones
- 10 Sindrome CompartimentalDocumento33 páginas10 Sindrome CompartimentalGeov Contreras100% (1)
- Insuficiencia CardiacaDocumento5 páginasInsuficiencia CardiacaCecy Frausto VelascoAún no hay calificaciones
- Premedicacion, Ayuno, Preparacion Anestesicos en PediatriaDocumento30 páginasPremedicacion, Ayuno, Preparacion Anestesicos en Pediatriakativana100% (1)
- Monitoreo de PicDocumento74 páginasMonitoreo de PicELy AbantoAún no hay calificaciones
- PicDocumento97 páginasPicDra Eliana NarváezAún no hay calificaciones
- Patologia Bloque 1 (Semana 1-4)Documento181 páginasPatologia Bloque 1 (Semana 1-4)Manuel Diaz EstradaAún no hay calificaciones
- PLANTILLASDocumento50 páginasPLANTILLASCarito Di CompostellaAún no hay calificaciones
- ENFERMEDAD RENAL CRONICA VVDocumento35 páginasENFERMEDAD RENAL CRONICA VVvivianaAún no hay calificaciones
- Teoria Semana 1 Estudio e Interprecion de HemogramaDocumento292 páginasTeoria Semana 1 Estudio e Interprecion de HemogramaErik J. Roshan FloresAún no hay calificaciones
- Artritis ReumatoideDocumento46 páginasArtritis ReumatoideNicole Medina VásquezAún no hay calificaciones
- Caso Clinico Anticoagulacion OdontoDocumento21 páginasCaso Clinico Anticoagulacion OdontoRicardo TorresAún no hay calificaciones
- Distres RespiratprioDocumento128 páginasDistres RespiratprioCarolina ArteagaAún no hay calificaciones
- Anestesia Cirugia LaparoscopicaDocumento24 páginasAnestesia Cirugia LaparoscopicaAylud RaimeAún no hay calificaciones
- Generalidades Procuración de Órgano SDocumento20 páginasGeneralidades Procuración de Órgano SDiosnena2096Aún no hay calificaciones
- Orden Medica en Urgencia DR Isaias Garcerant PDFDocumento69 páginasOrden Medica en Urgencia DR Isaias Garcerant PDFISAIAS3 GARCERANT CAMPO100% (1)
- Terapia Combinada en HtaDocumento55 páginasTerapia Combinada en HtaJulio SotoAún no hay calificaciones
- SobrecoagulacionDocumento55 páginasSobrecoagulacionChristian GarciaAún no hay calificaciones
- Recepcion Del Paciente Pos Operado de Cirugia Cardiaca FinalDocumento66 páginasRecepcion Del Paciente Pos Operado de Cirugia Cardiaca FinalELy AbantoAún no hay calificaciones
- Terapia RecompresivaDocumento31 páginasTerapia RecompresivaTelentis ZAún no hay calificaciones
- 6 Semana Caso Clinico Aborto ActualDocumento17 páginas6 Semana Caso Clinico Aborto ActualLuz Chumbiauca HuamaniAún no hay calificaciones
- Actuación Sanitaria en Emergencias NuclearesDocumento44 páginasActuación Sanitaria en Emergencias Nuclearescolate2Aún no hay calificaciones
- Caso Clinico. Giss BronquiolitisDocumento18 páginasCaso Clinico. Giss BronquiolitisGisa Indira PerezMitaAún no hay calificaciones
- Empo - Sanga Turpo Brian - Imco Servicios1Documento23 páginasEmpo - Sanga Turpo Brian - Imco Servicios1Anonymous ugqHW3Aún no hay calificaciones
- AsmaDocumento30 páginasAsmaMaria de los Angeles Garcia BautistaAún no hay calificaciones
- Oxigenación Cerebral PtO2 ClinicasMontevideoUy2019Documento50 páginasOxigenación Cerebral PtO2 ClinicasMontevideoUy2019Luis CruzAún no hay calificaciones
- Cruz Avila Rocio 1Documento2 páginasCruz Avila Rocio 1Faby MtzAún no hay calificaciones
- AlgoritmosoloDocumento3 páginasAlgoritmosoloCesar BarriosAún no hay calificaciones
- Codigo Sepsis Propuesta (Autosaved)Documento72 páginasCodigo Sepsis Propuesta (Autosaved)Jorge AzocarAún no hay calificaciones
- Miocardiopatia DiabeticaDocumento20 páginasMiocardiopatia DiabeticaRoy Christian Campos RequejoAún no hay calificaciones
- Manipulacion Minima Del Recien NacidoDocumento39 páginasManipulacion Minima Del Recien Nacidoyouaresolucky100% (8)
- Bronquiolitis Vs NeumoniaDocumento33 páginasBronquiolitis Vs NeumoniaKevin PesantezAún no hay calificaciones
- Manejo Inicial Del Politraumatizado Pediátrico - DR MolinaDocumento43 páginasManejo Inicial Del Politraumatizado Pediátrico - DR MolinaCandela GarciaAún no hay calificaciones
- Caso 2Documento22 páginasCaso 2Matias Adrián BianciottoAún no hay calificaciones
- Modelo de Evolucion ClinicaDocumento2 páginasModelo de Evolucion ClinicaMabel R. Moya OrtizAún no hay calificaciones
- Hemodinamia y RadioterapiaDocumento44 páginasHemodinamia y RadioterapiaNico:-P AcostaAún no hay calificaciones
- Grupo 2 HC UciDocumento23 páginasGrupo 2 HC UciSteven VásquezAún no hay calificaciones
- Reto de LiquidosDocumento36 páginasReto de LiquidosFranco100% (1)
- Evaluacion PreoperatoriaDocumento47 páginasEvaluacion PreoperatoriaVERONICA PARI TOLAAún no hay calificaciones
- EPICRISIS Hic PDFDocumento4 páginasEPICRISIS Hic PDFtramites nuevaeramatematic documentosAún no hay calificaciones
- Paro CardiacoDocumento68 páginasParo CardiacocneilamorenoAún no hay calificaciones
- UltrasonidoDocumento31 páginasUltrasonidoMelissa VillanuevaAún no hay calificaciones
- Estado Epileptico PediatricoDocumento30 páginasEstado Epileptico PediatricoAldo Sihuincha FloresAún no hay calificaciones
- Enfermedades Hipertensivas en El Embarazo: Dra. Annel Dannezza Zegarra Camacho 2021Documento15 páginasEnfermedades Hipertensivas en El Embarazo: Dra. Annel Dannezza Zegarra Camacho 2021api-561104576Aún no hay calificaciones
- Presión FisicoquímicaDocumento12 páginasPresión FisicoquímicaJosselin G Morales RojasAún no hay calificaciones
- Angina EstableDocumento2 páginasAngina EstableAlicia LopezAún no hay calificaciones
- Caso Clínico Angel 2Documento27 páginasCaso Clínico Angel 2David lopezAún no hay calificaciones
- Modelo de Epicrisis MedicaDocumento17 páginasModelo de Epicrisis MedicaSylvester Alcívar MuñozAún no hay calificaciones
- Manejo de Linfoma No Hodgkin Linfoma Del Manto (MCL)Documento9 páginasManejo de Linfoma No Hodgkin Linfoma Del Manto (MCL)Iris GzlzAún no hay calificaciones
- VALORACION TraumaDocumento31 páginasVALORACION TraumaMichell CruzAún no hay calificaciones
- Diagnosticos de Neumonia Todos 2Documento13 páginasDiagnosticos de Neumonia Todos 2joy252Aún no hay calificaciones
- INDUCCIONDocumento42 páginasINDUCCIONastrid carolina flores cabreraAún no hay calificaciones
- 1 Jimmy TacoDocumento15 páginas1 Jimmy Tacoita79Aún no hay calificaciones
- Anestesia RegionalDocumento4 páginasAnestesia Regionalita79Aún no hay calificaciones
- Infecciones Post NQDocumento73 páginasInfecciones Post NQita79Aún no hay calificaciones
- Tratamiento Farmacológico de Las TaquiarritmiasDocumento11 páginasTratamiento Farmacológico de Las Taquiarritmiasita79Aún no hay calificaciones
- Aminas SimpaticomiméticasDocumento1 páginaAminas Simpaticomiméticasita79100% (1)
- Aminas SimpaticomiméticasDocumento1 páginaAminas Simpaticomiméticasita79100% (1)
- AntibioticoterapiaDocumento36 páginasAntibioticoterapiaita79Aún no hay calificaciones
- Chakras y Enfermedades Con ImanesDocumento15 páginasChakras y Enfermedades Con ImanesFrancisco Anaya VilledaAún no hay calificaciones
- Vademecum Tercero Sabados-1Documento80 páginasVademecum Tercero Sabados-1YARLYAún no hay calificaciones
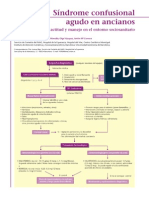
- Síndrome Confusional Agudo en Ancianos - Lorena BajoDocumento4 páginasSíndrome Confusional Agudo en Ancianos - Lorena BajoAnonymous x82e9Nb0Aún no hay calificaciones
- Info 008 Sso Primeros AuxiliosDocumento1 páginaInfo 008 Sso Primeros AuxiliosEidan RiveriAún no hay calificaciones
- Cuadro Comparativo Enfermedades Infeccionsa Elizabeth GarciaDocumento7 páginasCuadro Comparativo Enfermedades Infeccionsa Elizabeth Garciaelizabeth garciaAún no hay calificaciones
- Orzuelo y Chalazion PDFDocumento5 páginasOrzuelo y Chalazion PDFricardox28Aún no hay calificaciones
- Términos Semiológicos Del Aparato DigestivoDocumento9 páginasTérminos Semiológicos Del Aparato DigestivoCristian Aguirre Esparza50% (4)
- Diferencias en La Cicatrización de Las Heridas Cutaneas Entre Perros y GatosDocumento6 páginasDiferencias en La Cicatrización de Las Heridas Cutaneas Entre Perros y GatosAbel ArayaAún no hay calificaciones
- Tuberculosis e Infecciones Por Micobacterias AtípicasDocumento30 páginasTuberculosis e Infecciones Por Micobacterias AtípicasAbraham Martinez100% (1)
- AmebiasisDocumento75 páginasAmebiasisCraig BurgessAún no hay calificaciones
- Generalidades de TraumaDocumento37 páginasGeneralidades de TraumaPolux Cynthia MartzAún no hay calificaciones
- Guia de AinesDocumento3 páginasGuia de AinesCindy Maribel Lápez JarquínAún no hay calificaciones
- Estrategia de Atencion Al Pac CronicoDocumento102 páginasEstrategia de Atencion Al Pac CronicoIrene López ArenzanaAún no hay calificaciones
- Patogenia de Las ITUDocumento30 páginasPatogenia de Las ITUMarleni Beatriz OchicuaAún no hay calificaciones
- Gabriel Antonio Colamarco Ureña: Universidad San Francisco de QuitoDocumento37 páginasGabriel Antonio Colamarco Ureña: Universidad San Francisco de QuitoDanitza CervantesAún no hay calificaciones
- Indicaciones TerapéuticasDocumento5 páginasIndicaciones TerapéuticasGustavo SolisAún no hay calificaciones
- Datos de Filiación Del Menor y Datos FamiliaresDocumento8 páginasDatos de Filiación Del Menor y Datos FamiliaresJOHA CORNEJOAún no hay calificaciones
- Hoja Place Riesgo 1Documento2 páginasHoja Place Riesgo 1Anna Raquel FloresAún no hay calificaciones
- Enfermedades Del GustoDocumento3 páginasEnfermedades Del GustoJean Carlos Tejada100% (6)
- Cap14 PDFDocumento4 páginasCap14 PDFShawn GravesAún no hay calificaciones
- Hemorragias Del Primer TrimestreDocumento27 páginasHemorragias Del Primer Trimestrewilmar andradeAún no hay calificaciones
- Susana PaeDocumento19 páginasSusana PaeBrenda Yulipsa Reyes RomeroAún no hay calificaciones
- 206 Huesos Del CuerpoDocumento29 páginas206 Huesos Del Cuerpos4gorbalanAún no hay calificaciones
- Permiso Medico Yepez ChicaizaDocumento2 páginasPermiso Medico Yepez Chicaizacitas medicasAún no hay calificaciones
- Cardiología - BancoAnexo - Con ClavesDocumento8 páginasCardiología - BancoAnexo - Con ClavesKatherineAún no hay calificaciones