También podría gustarte
- Anestesiología GuíaDocumento110 páginasAnestesiología GuíaIatros Garcini100% (1)
- Farmacologia CardiovascularDocumento112 páginasFarmacologia CardiovascularEsther JaramilloAún no hay calificaciones
- Farmacología aplicada en anestesiología. Escenarios clínicosDe EverandFarmacología aplicada en anestesiología. Escenarios clínicosAún no hay calificaciones
- Bases para el manejo del paciente críticoDe EverandBases para el manejo del paciente críticoAún no hay calificaciones
- TesisDocumento130 páginasTesisCynthia HernandezAún no hay calificaciones
- ANTIVIRALESDocumento48 páginasANTIVIRALESGabriela Prado Gumiel100% (2)
- ANESTESIADocumento32 páginasANESTESIAVanesa Soledaad50% (2)
- Clínica de anestesia cardiovascular CMA Vol. 7De EverandClínica de anestesia cardiovascular CMA Vol. 7Aún no hay calificaciones
- SimpaticolíticosDocumento11 páginasSimpaticolíticosIvan Rivera100% (1)
- Farmacología de Los Anestésicos Generales y Locales: Práctica en Aula Semana #03Documento42 páginasFarmacología de Los Anestésicos Generales y Locales: Práctica en Aula Semana #03Cinthya CruzadoAún no hay calificaciones
- Red Latinoamericana para El Uso Seguro de Mx-2015Documento4 páginasRed Latinoamericana para El Uso Seguro de Mx-2015mariela maldonado escobedoAún no hay calificaciones
- Anestesia General PDFDocumento18 páginasAnestesia General PDFMiriam Doris Contreras AguilarAún no hay calificaciones
- Manejo Anestésico en Cirugía Hepática, Vía Biliar y de PáncreasDocumento12 páginasManejo Anestésico en Cirugía Hepática, Vía Biliar y de PáncreasBoris Hernandez AlejoAún no hay calificaciones
- Pharmacological Treatment of Obesity: Tratamiento Farmacológico de La ObesidadDocumento12 páginasPharmacological Treatment of Obesity: Tratamiento Farmacológico de La ObesidadJustina100% (1)
- 7-Articulo de Revision 2Documento6 páginas7-Articulo de Revision 2Jose luisAún no hay calificaciones
- Anestesio PDFDocumento27 páginasAnestesio PDFKarly Ayala CarrilloAún no hay calificaciones
- CirugiaDocumento36 páginasCirugiaPaulo Linares PercaAún no hay calificaciones
- Grupo 1. Anestesia GeneralDocumento53 páginasGrupo 1. Anestesia GeneralEzequiel PasasinAún no hay calificaciones
- Semana 4 Intraoperatorio-PabellonDocumento65 páginasSemana 4 Intraoperatorio-PabellonJannisel MartinezAún no hay calificaciones
- Trabalho Taty Semi ProntoDocumento10 páginasTrabalho Taty Semi ProntoDanillo Pinto de JesusAún no hay calificaciones
- ANESTESICOSDocumento50 páginasANESTESICOSEliana Rosero RualesAún no hay calificaciones
- Es - 0120 3347 Rca 46 02 93Documento5 páginasEs - 0120 3347 Rca 46 02 93ivanAún no hay calificaciones
- Awake Craniotomy Indications Benefits and TechniquDocumento7 páginasAwake Craniotomy Indications Benefits and TechniquJannely Butron MontañoAún no hay calificaciones
- Anestesia RegionalDocumento26 páginasAnestesia RegionalmiriamnavarrorizosAún no hay calificaciones
- 2448 8771 Am 30 03 20Documento18 páginas2448 8771 Am 30 03 20Javier Farias VeraAún no hay calificaciones
- Control Del Dolor Postoperatorio en Cirugía AbdominalDocumento4 páginasControl Del Dolor Postoperatorio en Cirugía AbdominalRaquel Guijarro MartinezAún no hay calificaciones
- Anestesia General InformeDocumento19 páginasAnestesia General InformeLenis C VasquesAún no hay calificaciones
- Tema 1 Modalidades de AnestesiaDocumento36 páginasTema 1 Modalidades de AnestesiaGAMBOA NICOLAS JOSE 201802350 ESTUDIANTEAún no hay calificaciones
- Grupo CTO - Asignatura - Resúmenes - T1 ANESTESIADocumento4 páginasGrupo CTO - Asignatura - Resúmenes - T1 ANESTESIACRISTINA DURÁN ÁVILAAún no hay calificaciones
- Anestesia para Cirugía de HombroDocumento12 páginasAnestesia para Cirugía de HombroAbisaid Jonathan Salinas MemijeAún no hay calificaciones
- Cix-02-G02 Guia de Anestesia RegionalDocumento19 páginasCix-02-G02 Guia de Anestesia RegionalalexAún no hay calificaciones
- Anestesia Equilibrada en Pequeñas EspeciesDocumento18 páginasAnestesia Equilibrada en Pequeñas EspeciesPickyukiAún no hay calificaciones
- Protocolo Dolor POP NHBGDocumento28 páginasProtocolo Dolor POP NHBGALFONSO MARTINEZ VISBALAún no hay calificaciones
- Anestesia COmbinadaDocumento6 páginasAnestesia COmbinadaHenry ManuelAún no hay calificaciones
- Anestesia Local y RegionalDocumento3 páginasAnestesia Local y RegionalMarcelo CobeñaAún no hay calificaciones
- Manejo Del Dolor en PlásticaDocumento2 páginasManejo Del Dolor en PlásticaChristian Morel SosaAún no hay calificaciones
- Interacciones de AnestesicosDocumento12 páginasInteracciones de AnestesicosYenny Gliseth TypeAún no hay calificaciones
- Caso Clinico - Formato PDFDocumento56 páginasCaso Clinico - Formato PDFJoseLainezAún no hay calificaciones
- 3 CTO Anestesiologia OncologiaDocumento24 páginas3 CTO Anestesiologia OncologiaChristel Gutierrez PimentelAún no hay calificaciones
- AnestesiaDocumento11 páginasAnestesiaCruz Elena Tovar Rodriguez0% (1)
- 2cir3-Ane-02!31!05 - Introduccion A La AnestesiologiaDocumento10 páginas2cir3-Ane-02!31!05 - Introduccion A La Anestesiologiamenfis cortezAún no hay calificaciones
- Anestesio T6Documento2 páginasAnestesio T6Fatima Burgos LopezAún no hay calificaciones
- PDF Anestesia VargasDocumento17 páginasPDF Anestesia Vargasximenna nicold vargas arriagaAún no hay calificaciones
- Periodo TRANSOPERATORIO TerminadoDocumento52 páginasPeriodo TRANSOPERATORIO TerminadoJherson Pacheco Guerrero50% (2)
- Cesaria y DolorDocumento11 páginasCesaria y DolorSantiago RomeraAún no hay calificaciones
- Anestesia y Analgesia Peridural Torácica para Cirugía OncológicaDocumento11 páginasAnestesia y Analgesia Peridural Torácica para Cirugía Oncológicasanjuandediosanestesia100% (3)
- Rr122cropivacaina Vs Fentanilo Bombas Elastomerica Post CirugiaDocumento11 páginasRr122cropivacaina Vs Fentanilo Bombas Elastomerica Post CirugiaalexanderAún no hay calificaciones
- Es - 0120 3347 Rca 46 03 257Documento5 páginasEs - 0120 3347 Rca 46 03 257Ambar Esquivel OcampoAún no hay calificaciones
- Farmacología Del Sistema Nervioso Central. AnestesicosDocumento12 páginasFarmacología Del Sistema Nervioso Central. AnestesicosLargion Jose HerreraAún no hay calificaciones
- Tipos de AnestesiaDocumento23 páginasTipos de AnestesiaELSA PAOLA TURRUBIATES CHANEZAún no hay calificaciones
- Capitulo 5 Tec AnestesicaDocumento19 páginasCapitulo 5 Tec AnestesicaCamiAchucarroAún no hay calificaciones
- Generalidades de Anestesia11Documento14 páginasGeneralidades de Anestesia111315608768zmzfAún no hay calificaciones
- Infusores IV en CX Plastica DosisDocumento6 páginasInfusores IV en CX Plastica DosisDaniel MarinAún no hay calificaciones
- AnestesiaDocumento2 páginasAnestesiaRosmeri NavarroAún no hay calificaciones
- ANESTESIOLOGÍADocumento54 páginasANESTESIOLOGÍAJuanita CepillinAún no hay calificaciones
- N° 11 AnestésicosDocumento12 páginasN° 11 AnestésicosSILVIA MEDALY CASTILLO RODRIGUEZAún no hay calificaciones
- Cuestionario de Medico QuirurgicaDocumento12 páginasCuestionario de Medico QuirurgicaERICK LEONARDO GRIMALDO PRETELAún no hay calificaciones
- 02-Ane-18-02-Anestesia General.Documento6 páginas02-Ane-18-02-Anestesia General.Daniel Alberto RojasAún no hay calificaciones
- Documento Sin TítuloDocumento4 páginasDocumento Sin TítuloPAOLA KATHERINE CORTÉS REYESAún no hay calificaciones
- Documento Sin TítuloDocumento4 páginasDocumento Sin TítuloPAOLA KATHERINE CORTÉS REYESAún no hay calificaciones
- Escaleno PosteriorDocumento6 páginasEscaleno PosteriorJuan Guillermo Llancari VargasAún no hay calificaciones
- Anestesia CXDocumento20 páginasAnestesia CXAna FisanottiAún no hay calificaciones
- ESTE3Documento6 páginasESTE3Sheilla Gomez TejadaAún no hay calificaciones
- Ha Farmaco inDocumento41 páginasHa Farmaco inMaria Alexandra Murcia OcampoAún no hay calificaciones
- La cirugía laparoscópica en el manejo de los principales padecimientos del aparato digestivo CGM 01De EverandLa cirugía laparoscópica en el manejo de los principales padecimientos del aparato digestivo CGM 01Aún no hay calificaciones
- ¿Cómo Se Trata El Cáncer de Cuello Uterino?Documento36 páginas¿Cómo Se Trata El Cáncer de Cuello Uterino?Alba LopezAún no hay calificaciones
- Captura de Pantalla 2023-04-30 A La(s) 9.12.11Documento43 páginasCaptura de Pantalla 2023-04-30 A La(s) 9.12.11Alba LopezAún no hay calificaciones
- InformeResultados1 047650Documento1 páginaInformeResultados1 047650Alba LopezAún no hay calificaciones
- InformeResultados1 047327Documento1 páginaInformeResultados1 047327Alba LopezAún no hay calificaciones
- Ecturacrtica ModelodeComunicacinHumanaDocumento9 páginasEcturacrtica ModelodeComunicacinHumanaAlba LopezAún no hay calificaciones
- Evaluación Aleatoria Del Intervalo de Tiempo Óptimo Entre Bolos Epidurales Intermitentes Programados Técnica para La Analgesia Del PartoDocumento8 páginasEvaluación Aleatoria Del Intervalo de Tiempo Óptimo Entre Bolos Epidurales Intermitentes Programados Técnica para La Analgesia Del PartoAlba LopezAún no hay calificaciones
- Generalidades de La Anestesia 10Documento16 páginasGeneralidades de La Anestesia 10Briseida Elizabeth ArreolaAún no hay calificaciones
- FENILBUTAZONA - MUSTAD ARGENTINA - Mustad Argentina S.A. - Antinflamatorios y Antihistaminicos - Vademecum Sani - Productos VeterinariosDocumento2 páginasFENILBUTAZONA - MUSTAD ARGENTINA - Mustad Argentina S.A. - Antinflamatorios y Antihistaminicos - Vademecum Sani - Productos VeterinariosedgarAún no hay calificaciones
- Alertas Sanitarias PDFDocumento3258 páginasAlertas Sanitarias PDFJuanqueAún no hay calificaciones
- Niveles de Evidencia Estudios de BridionDocumento4 páginasNiveles de Evidencia Estudios de BridionJuly Vianneth Torres GonzálezAún no hay calificaciones
- Presentación 1 MarihuanaDocumento6 páginasPresentación 1 Marihuanaicydiegoo θAún no hay calificaciones
- Analgesicos OpiaceosDocumento24 páginasAnalgesicos OpiaceoscarolAún no hay calificaciones
- Medicamentos y AlcoholDocumento3 páginasMedicamentos y AlcoholJulissa Alejandra Barturen SandovalAún no hay calificaciones
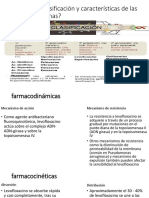
- ¿Cuál Es La Clasificación y Características de Las Fluoroquinolonas?Documento6 páginas¿Cuál Es La Clasificación y Características de Las Fluoroquinolonas?Jorge Diego Galvez FloresAún no hay calificaciones
- BICARBONATO 500 MG 100 CÁPSULAS PDFDocumento2 páginasBICARBONATO 500 MG 100 CÁPSULAS PDFMar RaAún no hay calificaciones
- De Origen VegetalDocumento4 páginasDe Origen VegetalAnonymous 45UzutFNkgAún no hay calificaciones
- Lotrial PrecioDocumento2 páginasLotrial PrecioheraclitodeefesoAún no hay calificaciones
- Medicamentos de Alto RiesgoDocumento7 páginasMedicamentos de Alto RiesgoAlejandra LópezAún no hay calificaciones
- Medicamentos Carro de Paro AgudosDocumento6 páginasMedicamentos Carro de Paro AgudosMaria Victoria DIAZ DIAZAún no hay calificaciones
- LLD Apixaban (Eliquis) Tablets CDS 19apr2019 CDS 27jun2019 v4Documento48 páginasLLD Apixaban (Eliquis) Tablets CDS 19apr2019 CDS 27jun2019 v4stevenjosea5802Aún no hay calificaciones
- Anestésicos Locales Tipo ÉsterDocumento13 páginasAnestésicos Locales Tipo ÉsterDavid CHAún no hay calificaciones
- Costos Lundbeck 2021Documento1 páginaCostos Lundbeck 2021David ParraAún no hay calificaciones
- Algoritmo para Tratar Los Síntomas Coreicos en La Enfermedad e HuntingtonDocumento1 páginaAlgoritmo para Tratar Los Síntomas Coreicos en La Enfermedad e HuntingtonVictor A. OrozcoAún no hay calificaciones
- Lección 1-EPD PDF - PDF PLANTA MEDICINALESDocumento22 páginasLección 1-EPD PDF - PDF PLANTA MEDICINALESsofia pachecoAún no hay calificaciones
- INSTANTDocumento6 páginasINSTANTAlejandro RamírezAún no hay calificaciones
- Lista de PreciosDocumento12 páginasLista de PreciosBryan MuñozAún no hay calificaciones
- Anestésicos Generales InyectablesDocumento37 páginasAnestésicos Generales InyectablesDiana Silva YoveraAún no hay calificaciones
- Analgesia Postoperatoria en Cirugía PediátriaDocumento6 páginasAnalgesia Postoperatoria en Cirugía PediátriaEsteban PuigduvíAún no hay calificaciones
- Guía para Entender Que Es El Kratom, Consumo y Efectos.Documento7 páginasGuía para Entender Que Es El Kratom, Consumo y Efectos.Humberto SosaAún no hay calificaciones
- Clase QuinolonasDocumento39 páginasClase QuinolonasmariaAún no hay calificaciones