También podría gustarte
- Manejo HerniasDocumento43 páginasManejo HerniasLuciana jaraAún no hay calificaciones
- Cirugía hepatobiliar en Colombia: Perspectiva para no olvidar la historiaDe EverandCirugía hepatobiliar en Colombia: Perspectiva para no olvidar la historiaAún no hay calificaciones
- OSTOMÍASDocumento21 páginasOSTOMÍASJuan Pablo Masías100% (2)
- Seminario Pared AbdominalDocumento35 páginasSeminario Pared Abdominalmarlin100% (1)
- Técnicas Quirúrgicas Del Estomago PDFDocumento10 páginasTécnicas Quirúrgicas Del Estomago PDFMaira RamirezAún no hay calificaciones
- Cirugía de UrgenciaDocumento4 páginasCirugía de UrgenciaJulieta Mena0% (1)
- Presentación 2Documento27 páginasPresentación 2vero1521100% (1)
- Hernioplastia InguinalDocumento14 páginasHernioplastia InguinalSantiago Rguez OrozcoAún no hay calificaciones
- Viscuso, Matías Nicolás - Hernia Inguinofemoral 2Documento12 páginasViscuso, Matías Nicolás - Hernia Inguinofemoral 2Matias Viscuso100% (1)
- Técnicas Quirúrgicas para Cirugía de TiroidesDocumento24 páginasTécnicas Quirúrgicas para Cirugía de TiroidesCesar Silva M100% (1)
- Viscuso, Matías Nicolás - Hernia Ventral PrimariaDocumento18 páginasViscuso, Matías Nicolás - Hernia Ventral PrimariaMatias ViscusoAún no hay calificaciones
- Hemicolectomia DerechaDocumento26 páginasHemicolectomia Derechapasaja15350% (1)
- ColostomíasDocumento12 páginasColostomíasElio Renzo Rimarachín Valderrama100% (2)
- GastroyeyunostomiaDocumento5 páginasGastroyeyunostomiaBrayan BarajasAún no hay calificaciones
- Tecnicas Quirurgicas en Los ProlapsosDocumento21 páginasTecnicas Quirurgicas en Los ProlapsosDiter SilvaAún no hay calificaciones
- Bypass Femoro-PopliteoDocumento10 páginasBypass Femoro-Popliteobetzabeth obregon araujoAún no hay calificaciones
- Tesis FinalDocumento40 páginasTesis FinalYoel Diaz La RataAún no hay calificaciones
- ESPLENECTOMIA 2019 FranchoDocumento43 páginasESPLENECTOMIA 2019 Franchoanon_121404482Aún no hay calificaciones
- TimectomiaDocumento26 páginasTimectomiaCarlos Elio Polo VargasAún no hay calificaciones
- Procedimientos QuirurgicosDocumento55 páginasProcedimientos QuirurgicosMonica Patricia Huamán Reyes100% (1)
- Incisionesdr 140401233134 Phpapp01Documento77 páginasIncisionesdr 140401233134 Phpapp01SolAún no hay calificaciones
- Video ToracosDocumento32 páginasVideo ToracosEitel Solano PerezAún no hay calificaciones
- Hemicolectomia LaparosDocumento19 páginasHemicolectomia LaparosYeys Ballesteros Guardo100% (1)
- Exploracion de Vias BiliaresDocumento8 páginasExploracion de Vias BiliaresEver Andres Zegarra CandiottiAún no hay calificaciones
- Gastro y Yeyuno TécnicaDocumento13 páginasGastro y Yeyuno TécnicaJuanjo ArceAún no hay calificaciones
- Cirugía HepáticaDocumento24 páginasCirugía Hepática127269100% (1)
- Técnicas Quirúrgicas Proctología Ant - Anato y T QX ProctoDocumento23 páginasTécnicas Quirúrgicas Proctología Ant - Anato y T QX ProctoErick Alejandro100% (1)
- Fistulas AnorrectalesDocumento10 páginasFistulas AnorrectalesJhon Antonio EspinozaAún no hay calificaciones
- Toracotomia Articulo de RevisionDocumento10 páginasToracotomia Articulo de RevisionmickypmAún no hay calificaciones
- Técnicas Quirúrgicas de Gastrocirugía CompletoDocumento48 páginasTécnicas Quirúrgicas de Gastrocirugía CompletoSara MtzAún no hay calificaciones
- LinfadenectomiaDocumento41 páginasLinfadenectomiajibrirchAún no hay calificaciones
- Hernias Ponencia MagistralDocumento39 páginasHernias Ponencia MagistralOscar Daniel Mera Ruiz100% (1)
- AnastomosisDocumento6 páginasAnastomosisJorge Ivan Neri CobosAún no hay calificaciones
- Técnicas Quirúrgicas 2021-2022Documento443 páginasTécnicas Quirúrgicas 2021-2022gaby Aguilar100% (1)
- Anastomosis IntestinalDocumento55 páginasAnastomosis Intestinalgeorge66500Aún no hay calificaciones
- Anatomia Quirurgica de La MamaDocumento39 páginasAnatomia Quirurgica de La MamaLaura MD100% (1)
- Manual QX 2Documento92 páginasManual QX 2Karla OrtizAún no hay calificaciones
- Tecnicas QX de EstomagoDocumento45 páginasTecnicas QX de Estomagoalejandrina100% (1)
- Trauma de Cuello-TraducidoDocumento16 páginasTrauma de Cuello-TraducidoValentina CastañedaAún no hay calificaciones
- Hernia Inguinal e HidroceleDocumento27 páginasHernia Inguinal e HidroceleDanna RincónAún no hay calificaciones
- Capitulo1 Guia Cirugia HepaticaDocumento18 páginasCapitulo1 Guia Cirugia HepaticaJuan_Brujo_8602Aún no hay calificaciones
- Traqueostomía Técnica QuirúrgicaDocumento74 páginasTraqueostomía Técnica Quirúrgicakenia escamillaAún no hay calificaciones
- Posiciones Quirurgicas Más HabitualesDocumento22 páginasPosiciones Quirurgicas Más Habitualesedwingiancarlo5912Aún no hay calificaciones
- Abordaje Quirurgico de AbdomenDocumento8 páginasAbordaje Quirurgico de AbdomenKristian BernalAún no hay calificaciones
- EnteroanastomosisDocumento49 páginasEnteroanastomosisIgnacio Cardenas Rodriguez100% (1)
- Simpatectomia Transtorácica EndoscópicaDocumento9 páginasSimpatectomia Transtorácica EndoscópicaLizeth SMAún no hay calificaciones
- 2002 Pilorotomía Extramucosa en El LactanteDocumento3 páginas2002 Pilorotomía Extramucosa en El LactanteJosé Luis Navarro RomeroAún no hay calificaciones
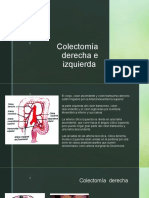
- Colectomia Derecha e IzquierdaDocumento10 páginasColectomia Derecha e IzquierdaOscar Benitez RamosAún no hay calificaciones
- LAPAROTOMIADocumento4 páginasLAPAROTOMIALuis Ivan Pineda Kunihiro100% (1)
- Pared Abdominal DificilDocumento23 páginasPared Abdominal DificilRamiro AlanisAún no hay calificaciones
- Equipo 5. Gastrostomia & GastrectomiaDocumento26 páginasEquipo 5. Gastrostomia & GastrectomiaAna Karen Barrera100% (1)
- Estrechez UretralDocumento17 páginasEstrechez UretralMemo Olivé100% (1)
- Avances en Cirugia LaparoscopicaDocumento46 páginasAvances en Cirugia LaparoscopicaIber CoutiñoAún no hay calificaciones
- CLASE 12 Laparoscopia - HisterectomíaDocumento70 páginasCLASE 12 Laparoscopia - HisterectomíaGyzary OspinaAún no hay calificaciones
- Apendicectomia, Cecostomia e Ileostomias.Documento58 páginasApendicectomia, Cecostomia e Ileostomias.cleanny espinozaAún no hay calificaciones
- Suturas Mecanicas y VacDocumento25 páginasSuturas Mecanicas y VacCarolina BermúdezAún no hay calificaciones
- Decisión en Laparoscopia: Introducción a la robóticaDe EverandDecisión en Laparoscopia: Introducción a la robóticaAún no hay calificaciones
- Estimacion IFG Atn PrimariaDocumento4 páginasEstimacion IFG Atn PrimariaPedro Espinosa HernándezAún no hay calificaciones
- 10.RIÑON y EMBARAZODocumento30 páginas10.RIÑON y EMBARAZOPedro Espinosa HernándezAún no hay calificaciones
- Aspectos Nutricionales ERCDocumento10 páginasAspectos Nutricionales ERCPedro Espinosa HernándezAún no hay calificaciones
- 8.glomerulonefritis AgudaDocumento25 páginas8.glomerulonefritis AgudaPedro Espinosa HernándezAún no hay calificaciones
- Manual de Ginecologia Y ObstetriciaDocumento195 páginasManual de Ginecologia Y ObstetriciaPedro Espinosa HernándezAún no hay calificaciones
- Anatomia Del CorazonDocumento77 páginasAnatomia Del CorazonMontserrat_Gon_8679Aún no hay calificaciones
- Alteraciones ElectroliticasDocumento27 páginasAlteraciones ElectroliticasPedro Espinosa HernándezAún no hay calificaciones
- Afecciones Vesícula BiliarDocumento51 páginasAfecciones Vesícula BiliarPedro Espinosa Hernández100% (1)
- Anatomia de CuelloDocumento46 páginasAnatomia de CuelloPedro Espinosa Hernández100% (1)
- Lesiones Musculoesqueleticas en OdontologiaDocumento8 páginasLesiones Musculoesqueleticas en OdontologiaEladio CossioAún no hay calificaciones
- Asepsia y AntisepsiaDocumento62 páginasAsepsia y AntisepsiaClaude BastienAún no hay calificaciones
- Diapositivas Revisadas Del Proyecto 2014Documento36 páginasDiapositivas Revisadas Del Proyecto 2014elmer garcia huarangaAún no hay calificaciones
- Definición de Vejiga NeurogenaDocumento3 páginasDefinición de Vejiga NeurogenaedjimonAún no hay calificaciones
- Crecl AphDocumento6 páginasCrecl Aphlenn75Aún no hay calificaciones
- Sentencia Grita SilencioDocumento36 páginasSentencia Grita SilencioAnonymous 0rdfosSTYSAún no hay calificaciones
- Esqueleto Del TroncoDocumento56 páginasEsqueleto Del TroncoAdriana RodriguezAún no hay calificaciones
- Ejercicios para La Artrosis de RodillaDocumento6 páginasEjercicios para La Artrosis de RodillaAna Paula Paredes100% (1)
- Primeros Auxilios - RCPDocumento98 páginasPrimeros Auxilios - RCPBofonoAún no hay calificaciones
- Trastornos de La Articulacion TemporomandibularDocumento7 páginasTrastornos de La Articulacion TemporomandibularRaul TorricoAún no hay calificaciones
- Recordatorio AnatómicoDocumento6 páginasRecordatorio AnatómicoEfrain Einer Condori NestasAún no hay calificaciones
- Primeros AuxiliosDocumento40 páginasPrimeros AuxiliosNelson de Castro - Ritmos y Dance ProjectAún no hay calificaciones
- Caso Análisis - Evento AdversoDocumento3 páginasCaso Análisis - Evento AdversoPaula Dueñas100% (1)
- Troncos: DivisionesDocumento4 páginasTroncos: DivisionesSteve AnguloAún no hay calificaciones
- 4 Carpeta, Articulaciones en AdelanteDocumento22 páginas4 Carpeta, Articulaciones en AdelanteE GAún no hay calificaciones
- NeumotoraxDocumento2 páginasNeumotoraxEmy Xavier KingAún no hay calificaciones
- Control de Daños en ObstetriciaDocumento6 páginasControl de Daños en ObstetriciaMagic_Over100% (1)
- Equipo 6 Síndrome Neurona Motora Sup e InfDocumento25 páginasEquipo 6 Síndrome Neurona Motora Sup e InfRuth Cobo Rosales0% (2)
- Mordida Cruzada Localizada Bilateral UnilateralDocumento18 páginasMordida Cruzada Localizada Bilateral UnilateralLeidyVanessaJaimesTolozaAún no hay calificaciones
- SECUENCIA DLM Cuerpo Completo Versión 1.0Documento15 páginasSECUENCIA DLM Cuerpo Completo Versión 1.0noemi floresAún no hay calificaciones
- Enf - ESCLEROSIS MÚLTIPLEDocumento10 páginasEnf - ESCLEROSIS MÚLTIPLEDANIEL ALEJANDROAún no hay calificaciones
- Trauma Raquimedular Presentacion FinalDocumento42 páginasTrauma Raquimedular Presentacion FinalJuan R Hernandez LozanoAún no hay calificaciones
- Radiologia Veterinaria Caninos y Felinos - Dra Patricia EscarateDocumento70 páginasRadiologia Veterinaria Caninos y Felinos - Dra Patricia Escarateleono856_vizcarra0% (1)
- P. AuxiliosDocumento28 páginasP. Auxiliosluis fernando alean mezaAún no hay calificaciones
- Hernias y EventracionesDocumento28 páginasHernias y EventracionesJoseCamposAún no hay calificaciones
- Miembro Superior Completo - Presentación DefinitivaDocumento117 páginasMiembro Superior Completo - Presentación DefinitivaJean PantojaAún no hay calificaciones
- Pia 201Documento123 páginasPia 201NICOLÁS ANDRÉS AYELEF PARRAGUEZAún no hay calificaciones
- Lesion EsfenobasilarDocumento41 páginasLesion Esfenobasilarmauricio rodriguezAún no hay calificaciones
- 4.2. Vocabulario QuechuaDocumento3 páginas4.2. Vocabulario QuechuaMisael GuillénAún no hay calificaciones
- Dossier Memoria PDFDocumento78 páginasDossier Memoria PDFdanielaAún no hay calificaciones