También podría gustarte
- Guía de evaluación auditiva en atención primaria. Un enfoque para el primer nivel de atenciónDe EverandGuía de evaluación auditiva en atención primaria. Un enfoque para el primer nivel de atenciónAún no hay calificaciones
- Índice de Discapacidad VocalDocumento2 páginasÍndice de Discapacidad VocalAny Castro0% (1)
- Anamnesis auditiva para trabajadores expuestos a ruidoDe EverandAnamnesis auditiva para trabajadores expuestos a ruidoAún no hay calificaciones
- Tratamiento DeglutorioDocumento33 páginasTratamiento DeglutorioSilvia de TorresAún no hay calificaciones
- Cuestionario en EspañolDocumento1 páginaCuestionario en EspañolLuis Guillermo Urra MarinAún no hay calificaciones
- RUBRICA13Documento1 páginaRUBRICA13Ivett-e Castro MoreiraAún no hay calificaciones
- Tendencia FisiológicaDocumento14 páginasTendencia FisiológicaimobliviateAún no hay calificaciones
- Fonoaudiología y Salud PúblicaDocumento11 páginasFonoaudiología y Salud PúblicaJorge Sandoval VargasAún no hay calificaciones
- Escala de Sintomas Vocales ESVDocumento2 páginasEscala de Sintomas Vocales ESVMartin Velasco CastroAún no hay calificaciones
- Nivel SemánticoDocumento29 páginasNivel SemánticoHelen Monsalves EspinozaAún no hay calificaciones
- Paper Estroboscopia 1Documento21 páginasPaper Estroboscopia 1Francisca Ruiz SalvoAún no hay calificaciones
- Hoja de Registro Pecfo CompressDocumento3 páginasHoja de Registro Pecfo CompressAmandaAún no hay calificaciones
- Capitulo 13 Mara Behlau PDFDocumento171 páginasCapitulo 13 Mara Behlau PDFSergio Morales EscalonaAún no hay calificaciones
- Datos Normativos de La VozDocumento10 páginasDatos Normativos de La VozAny CastroAún no hay calificaciones
- Cuestionario MiofuncionalDocumento11 páginasCuestionario MiofuncionalWendy MartinAún no hay calificaciones
- Resumen DisfoniasDocumento43 páginasResumen Disfoniasferbando1986Aún no hay calificaciones
- Guía Práctica Praat PDFDocumento7 páginasGuía Práctica Praat PDFjuan moreiraAún no hay calificaciones
- Clase 5 IF Lenguaje Niño Intervención Nivel Léxico SemanticoDocumento15 páginasClase 5 IF Lenguaje Niño Intervención Nivel Léxico SemanticoTamara Castillo100% (1)
- Disfonia MusculotensionalDocumento34 páginasDisfonia MusculotensionalMaterial Fonoaudiologico Rayito de Luz100% (4)
- Ejercicios FoniatriaDocumento3 páginasEjercicios FoniatriaMarzzia Meza ParedesAún no hay calificaciones
- Aplicación de La CIF A Los Trastornos Del Habla y Deglución en El AdultoDocumento10 páginasAplicación de La CIF A Los Trastornos Del Habla y Deglución en El Adultotolouc0% (1)
- Cuadro Resumen Disfonia Del CantanteDocumento2 páginasCuadro Resumen Disfonia Del CantanteMarianella Antonieta QCAún no hay calificaciones
- EvalVozFormatoDocumento6 páginasEvalVozFormatoOtnelup AbesAún no hay calificaciones
- Protocolo Evaluación RespiratoriaDocumento2 páginasProtocolo Evaluación RespiratoriaMegan MartinAún no hay calificaciones
- Analisis Acustico UvmDocumento55 páginasAnalisis Acustico UvmPriscilla NicolettAún no hay calificaciones
- I Ndice de Incapacidad Vocal - CantantesDocumento1 páginaI Ndice de Incapacidad Vocal - CantantesNadim Haddad MansillaAún no hay calificaciones
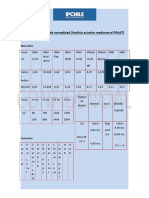
- Valores de Normalidad PRAATDocumento2 páginasValores de Normalidad PRAATConstanza Vargas GonzálezAún no hay calificaciones
- Pruebas SupraliminaresDocumento73 páginasPruebas SupraliminaresSOFIA CATALINA CORTES VELASQUEZAún no hay calificaciones
- Potenciales miogénicos evocados vestibularesDocumento22 páginasPotenciales miogénicos evocados vestibularesSamantha GuerraAún no hay calificaciones
- Daniela Jofre Teoria Fuente y FiltroDocumento17 páginasDaniela Jofre Teoria Fuente y FiltroDanito André JofréAún no hay calificaciones
- Calentamiento y Descalentamiento Vocal Oriana.....Documento2 páginasCalentamiento y Descalentamiento Vocal Oriana.....francisca caceresAún no hay calificaciones
- Técnicas de La TAVDocumento9 páginasTécnicas de La TAVgrace prambsAún no hay calificaciones
- Evaluación perceptual de la voz disfónica con la escala GRABSDocumento10 páginasEvaluación perceptual de la voz disfónica con la escala GRABSimAún no hay calificaciones
- Clase 8 - Maniobras y Compensaciones DeglutoriasDocumento40 páginasClase 8 - Maniobras y Compensaciones DeglutoriasDanae Miranda paredesAún no hay calificaciones
- Informe Audiología EvaluaciónDocumento2 páginasInforme Audiología EvaluaciónMayra TeránAún no hay calificaciones
- Registro anamnesis audiologíaDocumento4 páginasRegistro anamnesis audiologíaCatalina Muñoz CastilloAún no hay calificaciones
- ApraxiaDocumento5 páginasApraxiaKarina Andrea Jiménez CartesAún no hay calificaciones
- Evaluacion Funcional de La VozDocumento26 páginasEvaluacion Funcional de La VozSandra MuñozAún no hay calificaciones
- Poster TCCDocumento1 páginaPoster TCCjacque0318Aún no hay calificaciones
- Desarrollo del nivel léxico-semánticoDocumento28 páginasDesarrollo del nivel léxico-semánticoEstefani Romero ArriagadaAún no hay calificaciones
- PromociÓn en La Salud Vocal de Los Docentes A Partir de Un Estudio FonoergonomicoDocumento18 páginasPromociÓn en La Salud Vocal de Los Docentes A Partir de Un Estudio FonoergonomicoNicole Stephanie Martel MoralesAún no hay calificaciones
- Exploracion AerodinamicaDocumento3 páginasExploracion AerodinamicacnqjniqeiurjfnAún no hay calificaciones
- Prótesis Auditiva Intervención y RehabilitaciónDocumento4 páginasPrótesis Auditiva Intervención y RehabilitaciónBofor Aguilera100% (1)
- Dominio Del Fonoaudiólogo para La Determinación Del Grado de Viscosidad de Alimentos LíquidosDocumento11 páginasDominio Del Fonoaudiólogo para La Determinación Del Grado de Viscosidad de Alimentos LíquidosMatias OlguinAún no hay calificaciones
- Protocolos de Evaluación Del Adulto y Adulto Mayor: ManualdelfonoDocumento39 páginasProtocolos de Evaluación Del Adulto y Adulto Mayor: ManualdelfonocamilaAún no hay calificaciones
- Plan Terapuetico JosefaDocumento3 páginasPlan Terapuetico JosefaFelipe Jara FernandezAún no hay calificaciones
- Resultado Notas PsicometricasDocumento26 páginasResultado Notas PsicometricasEDWIN ARGENIS TIPAN RECALDEAún no hay calificaciones
- Anamnesis Voz Profesional 2Documento5 páginasAnamnesis Voz Profesional 2Sarita Fuentes NeedhamAún no hay calificaciones
- Disfagia HospitalDocumento82 páginasDisfagia HospitalCarmen Castillo Requena100% (1)
- Factores de Riesgo Vocal en Locutores de La Unidad de PatrullaDocumento22 páginasFactores de Riesgo Vocal en Locutores de La Unidad de PatrullaAlejandro Rodriguez-Cerna100% (1)
- Rehabilitacion Vocal TvsoDocumento2 páginasRehabilitacion Vocal Tvsorehabilitacion hcraAún no hay calificaciones
- Bonet Rehab Sord Adulto PDFDocumento3 páginasBonet Rehab Sord Adulto PDFjeannette molinaAún no hay calificaciones
- Cuidados Paliativos en Fonoaudiología y Ayudas Auditivas No ImplantablesDocumento4 páginasCuidados Paliativos en Fonoaudiología y Ayudas Auditivas No ImplantablesAngie CabreraAún no hay calificaciones
- Test de Evaluación Del Lenguaje Por NivelesDocumento8 páginasTest de Evaluación Del Lenguaje Por NivelesdanielaAún no hay calificaciones
- LABORATORIO 3 Amelia CortesDocumento4 páginasLABORATORIO 3 Amelia CortesmyristikAún no hay calificaciones
- Evaluación de la capacidad de comprensión del lenguaje hablado mediante logoaudiometríaDocumento15 páginasEvaluación de la capacidad de comprensión del lenguaje hablado mediante logoaudiometríaNatalia ArancibiaAún no hay calificaciones
- Afasia de WernickeDocumento13 páginasAfasia de WernickeTierradosAún no hay calificaciones
- Protocolo Pacientes Con Sintomas de DCM PDFDocumento2 páginasProtocolo Pacientes Con Sintomas de DCM PDFsardinetaAún no hay calificaciones
- Voice Handicap Index (Vhi) : Apartado para RehabilitacionDocumento1 páginaVoice Handicap Index (Vhi) : Apartado para RehabilitacionkariisaurioAún no hay calificaciones
- Parte I - F (Funcional) : Voice Handicap Index (Vhi)Documento2 páginasParte I - F (Funcional) : Voice Handicap Index (Vhi)JavieraAún no hay calificaciones
- Las Maracas Como Instrumento Musical UcDocumento78 páginasLas Maracas Como Instrumento Musical UcMiriamAún no hay calificaciones
- Paso3 Grupo7Documento9 páginasPaso3 Grupo7Diego BermúdezAún no hay calificaciones
- Tarea 5 Violencia de Genero JTCDocumento7 páginasTarea 5 Violencia de Genero JTCAna Laura Lara SantiagoAún no hay calificaciones
- Informe General Del Módulo IntroductorioDocumento58 páginasInforme General Del Módulo IntroductorioJimena rodriguez100% (2)
- Capitulo 09 Análisis de Correlación Lineal SimpleDocumento26 páginasCapitulo 09 Análisis de Correlación Lineal SimpleMiguel MalpartidaAún no hay calificaciones
- Trabajo de InvestigacionDocumento34 páginasTrabajo de InvestigacionBrandon Ulloa AvalosAún no hay calificaciones
- 18 Moral, Ética y BioéticaDocumento6 páginas18 Moral, Ética y BioéticaJulieta PerottiAún no hay calificaciones
- R4 - U3 UvegDocumento5 páginasR4 - U3 UvegmauricioleyvaperezAún no hay calificaciones
- Ejerc Propuestos de ProbabilidadesDocumento2 páginasEjerc Propuestos de ProbabilidadesAnonymous bPJvfkcgO3Aún no hay calificaciones
- Stand Up Comedy VenezuelaDocumento35 páginasStand Up Comedy VenezuelaBrunoAún no hay calificaciones
- Actividad Taller 4.3Documento19 páginasActividad Taller 4.3Stephanie PulecioAún no hay calificaciones
- Capítulo 2 TallerDocumento6 páginasCapítulo 2 TallerAleRodeaAún no hay calificaciones
- Enfoques de La Investigacion Cualitativa NovDocumento13 páginasEnfoques de La Investigacion Cualitativa NovmarisolAún no hay calificaciones
- Gestión de conflictosDocumento9 páginasGestión de conflictospaola0% (1)
- Prueba Escrita de Conocimientos 3 Dioses McoDocumento20 páginasPrueba Escrita de Conocimientos 3 Dioses McoAMERICA MICHELLE DEL ANGEL TORRESAún no hay calificaciones
- Estructura de Un Protocolo de InvestigaciónDocumento3 páginasEstructura de Un Protocolo de InvestigaciónRicardo H Rocha100% (1)
- ModeloDocumento11 páginasModeloLópez EnriqueAún no hay calificaciones
- Discusión 1 07092018-1Documento2 páginasDiscusión 1 07092018-1Chato Alarcon Charlaix0% (1)
- Topografía Taller No. 1Documento12 páginasTopografía Taller No. 1Gabela PinzonAún no hay calificaciones
- Informe #1 Biología 24-04-2019Documento3 páginasInforme #1 Biología 24-04-2019Andres VargasAún no hay calificaciones
- Conservación de la energía mecánicaDocumento7 páginasConservación de la energía mecánicaOSCAR LUIS GARRIDO ROJASAún no hay calificaciones
- SPA Formulación y Presentación de EEFF 2018-IIDocumento17 páginasSPA Formulación y Presentación de EEFF 2018-IIJohn AndersonAún no hay calificaciones
- Practica 1Documento9 páginasPractica 1Raul Bernabé TrejoAún no hay calificaciones
- Evolución histórica de las fuentes demográficasDocumento17 páginasEvolución histórica de las fuentes demográficasideucaAún no hay calificaciones
- Ejercicios de Estadistica 1 Febrero 2,014Documento3 páginasEjercicios de Estadistica 1 Febrero 2,014yalide50% (2)
- Ejercicios de ProbabilidadesDocumento50 páginasEjercicios de ProbabilidadesStephanie Mishell CondoriAún no hay calificaciones
- Solucion Caso Practico 2Documento3 páginasSolucion Caso Practico 2Juan PalacioAún no hay calificaciones
- YASHIRADocumento5 páginasYASHIRAYashira Estefany Valenzuela VeraAún no hay calificaciones
- Cognitivismo en Vzla.Documento11 páginasCognitivismo en Vzla.luis medinaAún no hay calificaciones
- Bioetica Tarea 3Documento4 páginasBioetica Tarea 3José Luis Alonso EscamillaAún no hay calificaciones