También podría gustarte
- Fundamentos de Las Enfermedades Del Tórax Tercera Edición RichardDocumento983 páginasFundamentos de Las Enfermedades Del Tórax Tercera Edición Richardoscarbarcenas417100% (1)
- Guía Teorica Extensiones de PestañasDocumento11 páginasGuía Teorica Extensiones de PestañaslauraethanmatAún no hay calificaciones
- Programación y Modos VNI UNABDocumento39 páginasProgramación y Modos VNI UNABMartïna AntonïaAún no hay calificaciones
- Tratamiento Kinesico RespiratorioDocumento8 páginasTratamiento Kinesico RespiratorioHernán Norambuena González0% (1)
- Guia de Practica Clinica AsmaDocumento20 páginasGuia de Practica Clinica Asmastefany100% (1)
- Asv PDFDocumento12 páginasAsv PDFErika GómezAún no hay calificaciones
- VM NeonatalDocumento8 páginasVM NeonatalWalter Huacani HuamaniAún no hay calificaciones
- Volumen - Garantizado 2008 Chile W Osorio PDFDocumento3 páginasVolumen - Garantizado 2008 Chile W Osorio PDFHoracio RogeAún no hay calificaciones
- Oxigenoterapia 2018 PDFDocumento31 páginasOxigenoterapia 2018 PDFkairosloco123Aún no hay calificaciones
- Algoritmos AHA 2020Documento13 páginasAlgoritmos AHA 2020Verónica Duménez Jofré100% (1)
- Manejo de La Vía Áerea en Pacientes Con Masas Cervicales 195117787009Documento7 páginasManejo de La Vía Áerea en Pacientes Con Masas Cervicales 195117787009Eugenio Martinez HurtadoAún no hay calificaciones
- VM en ObesosDocumento38 páginasVM en ObesosmarcosAún no hay calificaciones
- Bellanicurso 2Documento43 páginasBellanicurso 2Horacio RogeAún no hay calificaciones
- Fisiologìa RespiratoriaDocumento79 páginasFisiologìa RespiratoriaItzel Elizalde100% (1)
- PEEP en Diversos EscenariosDocumento24 páginasPEEP en Diversos Escenariosadrian mendoza croesAún no hay calificaciones
- Movimientos Elementales ComplejosbeksodbsDocumento80 páginasMovimientos Elementales ComplejosbeksodbsSánchez Mendiola Itzel GuadalupeAún no hay calificaciones
- Cementacion OseaDocumento5 páginasCementacion OseaBrenda FloresAún no hay calificaciones
- Destete de La Ventilacion MecanicaDocumento38 páginasDestete de La Ventilacion MecanicaJorge GMAún no hay calificaciones
- TECNICAS KINESICAS KinesioRESPDocumento4 páginasTECNICAS KINESICAS KinesioRESPBrandon Miler Guzman GragedaAún no hay calificaciones
- ParasitologíaDocumento29 páginasParasitologíaDiego CastroAún no hay calificaciones
- Actualización en CNAFDocumento97 páginasActualización en CNAFEduardo Tognarelli GuzmánAún no hay calificaciones
- Gestion Ventilación UnipulmonarDocumento31 páginasGestion Ventilación UnipulmonarJuan Sebastian TrujilloAún no hay calificaciones
- AerosolterapiaDocumento64 páginasAerosolterapiaDaniel Roa Bahamondes100% (2)
- Ejercicio Gases Arteriales PDFDocumento3 páginasEjercicio Gases Arteriales PDFvalentina garciaAún no hay calificaciones
- Rehabilitacion RespiratoriaDocumento28 páginasRehabilitacion RespiratoriaIsaac AC100% (1)
- SDR Neonatal Ur 2017Documento68 páginasSDR Neonatal Ur 2017Julián Camilo Torres EAún no hay calificaciones
- PROPOFOLDocumento91 páginasPROPOFOLAlexander BarriosnuevoAún no hay calificaciones
- DocMar FisioRespDocumento20 páginasDocMar FisioRespGuille Martin100% (1)
- Doppler Transcraneal en HsaDocumento70 páginasDoppler Transcraneal en Hsaoscar100% (1)
- Tcnicaskinsicasrespiratorias 120411191959 Phpapp02Documento32 páginasTcnicaskinsicasrespiratorias 120411191959 Phpapp02david8626100% (1)
- VortexDocumento9 páginasVortexAlfredoNoriegaPonceeAún no hay calificaciones
- Asincronía en La Ventilación Mecánica. Conceptos ActualesDocumento7 páginasAsincronía en La Ventilación Mecánica. Conceptos ActualesAngie MirandaAún no hay calificaciones
- Examen Fisico Del Aparato RespiratorioDocumento78 páginasExamen Fisico Del Aparato RespiratorioEstephany MolinaAún no hay calificaciones
- CNAFDocumento40 páginasCNAFCarlos LuqueAún no hay calificaciones
- Ventilacion Mecanica SERIE IDocumento23 páginasVentilacion Mecanica SERIE IIvan Osorio RuizAún no hay calificaciones
- Asincronia SATIDocumento70 páginasAsincronia SATINicolás HerreraAún no hay calificaciones
- Modos de Ventilacion MecanicaDocumento68 páginasModos de Ventilacion MecanicaEdison Alejandro Bonilla HaroAún no hay calificaciones
- Anestesia Raquídea EmcDocumento21 páginasAnestesia Raquídea Emckone80100% (2)
- Protocolo Manejo Respiratorio PDFDocumento18 páginasProtocolo Manejo Respiratorio PDFCamila Fernanda Rivera ArayaAún no hay calificaciones
- Manejo de Las Vías Respiratorias. Anestesia Clínica - Tratado BarashDocumento83 páginasManejo de Las Vías Respiratorias. Anestesia Clínica - Tratado BarashHenry CruelAún no hay calificaciones
- Maniobras de Reclutamiento AlveolarDocumento28 páginasManiobras de Reclutamiento Alveolarjohan perezAún no hay calificaciones
- Ventilación Mecánica 2Documento62 páginasVentilación Mecánica 2souls0693100% (1)
- Manejo Anestésico en Enfermedad Hepática-Sesion SARTD-CHGUV-11-6-18Documento42 páginasManejo Anestésico en Enfermedad Hepática-Sesion SARTD-CHGUV-11-6-18Karla DominguezAún no hay calificaciones
- Tarjetas Ventilacion MecanicaDocumento17 páginasTarjetas Ventilacion MecanicaPalomares Encinas Kevin100% (2)
- Anestesia en Paciente Crítico PDFDocumento7 páginasAnestesia en Paciente Crítico PDFJaviVillena100% (1)
- Gafas de Alto Flujo en Adulto PDFDocumento16 páginasGafas de Alto Flujo en Adulto PDFenfermeriaucihsjdaAún no hay calificaciones
- Intubación Bronquial SelectivaDocumento10 páginasIntubación Bronquial SelectivaEduardo Mercado Castro100% (1)
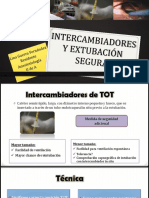
- Intercambiadores y Extubación SeguraDocumento42 páginasIntercambiadores y Extubación Seguraarthom100% (1)
- Monitoreo Hemodinámico 12Documento106 páginasMonitoreo Hemodinámico 12paola ignacio garciaAún no hay calificaciones
- Prono en Paciente Con SDRADocumento16 páginasProno en Paciente Con SDRAJavier Enrique Barrera PachecoAún no hay calificaciones
- Intubación Endotraqueal y TraqueostomíaDocumento9 páginasIntubación Endotraqueal y TraqueostomíaBeatriz LunaAún no hay calificaciones
- Posibles Complicaciones Tras La Cirugia Con Circulacion ExtracorporeaDocumento5 páginasPosibles Complicaciones Tras La Cirugia Con Circulacion ExtracorporeaAndrés Flores Fornés100% (1)
- Como Calcular El Flujo Inspiratorio STRDocumento2 páginasComo Calcular El Flujo Inspiratorio STRMarcelo Ortiz ValenzuelaAún no hay calificaciones
- LaringosDocumento80 páginasLaringosJuanPabloCamargoAún no hay calificaciones
- Efectos Sistemicos Ventilacion MecanicaDocumento24 páginasEfectos Sistemicos Ventilacion MecanicaBrenda de la Mora100% (1)
- Farmacología aplicada en anestesiología. Escenarios clínicosDe EverandFarmacología aplicada en anestesiología. Escenarios clínicosAún no hay calificaciones
- Breathing - Basic ARDS - L Munshi - No Animations TraducciónDocumento19 páginasBreathing - Basic ARDS - L Munshi - No Animations TraducciónMary GalvánAún no hay calificaciones
- Ventilación Mecanica Minsal 2012Documento21 páginasVentilación Mecanica Minsal 2012Christian Alonqueo100% (2)
- NeonatologíaDocumento36 páginasNeonatologíamarielamagnaboscoAún no hay calificaciones
- Fase BiofarmaceuticaDocumento28 páginasFase BiofarmaceuticaJennifer Salas CifuentesAún no hay calificaciones
- HNE LeishmaniasisDocumento3 páginasHNE LeishmaniasisMusica Sin CopyrightAún no hay calificaciones
- I PARCIAL Primeros AuxiliosDocumento5 páginasI PARCIAL Primeros AuxiliosMariaClaudiaDLeonAún no hay calificaciones
- Test de CribadoDocumento48 páginasTest de Cribadosandra milena100% (2)
- Caso Clinico Implante en Paciente Consumidor de BifosfonatosDocumento65 páginasCaso Clinico Implante en Paciente Consumidor de Bifosfonatoslorena8804Aún no hay calificaciones
- REQUERIMIENTO DE INSUMOS para El Año 2022Documento3 páginasREQUERIMIENTO DE INSUMOS para El Año 2022Mario Arevalo100% (2)
- 2 3 Movimientos Torax AbdomenCDocumento30 páginas2 3 Movimientos Torax AbdomenCClaudia Saldaña VillegasAún no hay calificaciones
- Hiponatremia NeonatalDocumento3 páginasHiponatremia NeonatalalejandraperezcastellarAún no hay calificaciones
- Lóbulos Del CerebroDocumento40 páginasLóbulos Del CerebrotalíaAún no hay calificaciones
- Evaluación y Diagnóstico en AdolescentesDocumento4 páginasEvaluación y Diagnóstico en AdolescentesOrlando Del Rosario PacherresAún no hay calificaciones
- Codigos SagradosDocumento10 páginasCodigos SagradosWalter Serrato100% (1)
- Cartilla OsdeDocumento398 páginasCartilla OsdePaula AndreaAún no hay calificaciones
- Caso Clínico CifDocumento5 páginasCaso Clínico Cifdavidarellano1992Aún no hay calificaciones
- Ficha de Ingreso Programa de Actividad FísicaDocumento2 páginasFicha de Ingreso Programa de Actividad FísicaSergio GarzónAún no hay calificaciones
- Ley N 1 de 10 de ENERODocumento12 páginasLey N 1 de 10 de ENEROCarmen Janeth De LeónAún no hay calificaciones
- Carta Descriptiva - Manejo Extintores PDFDocumento5 páginasCarta Descriptiva - Manejo Extintores PDFCarlos Chi100% (1)
- Farmacos AntiprotozoariosDocumento12 páginasFarmacos AntiprotozoariosMaria Concepción Chura BarónAún no hay calificaciones
- Familia-NeisseriaceaeDocumento47 páginasFamilia-NeisseriaceaecasulasamAún no hay calificaciones
- Teoría Del BigDocumento2 páginasTeoría Del BigmargaritaAún no hay calificaciones
- Manual Autismo - Colombia PDFDocumento152 páginasManual Autismo - Colombia PDFana rodriguezAún no hay calificaciones
- Taller Sistema Excretor Humano 45Documento3 páginasTaller Sistema Excretor Humano 45JuanGuillermoUruetaSierra100% (1)
- Normas VancouverDocumento9 páginasNormas VancouverManuel Gonzales BautistaAún no hay calificaciones
- Llamado General 2023Documento1 páginaLlamado General 2023Diana CarolinaAún no hay calificaciones
- Negligencia MedicaDocumento12 páginasNegligencia Medicaafanoso100% (2)
- Repaso 1er ParcialDocumento31 páginasRepaso 1er ParcialAndrés GRAún no hay calificaciones
- Ensayo (1) Riesgo ElectricoDocumento6 páginasEnsayo (1) Riesgo ElectricoBrenda FontalvoAún no hay calificaciones
- Las Gemas MedicinalesDocumento0 páginasLas Gemas MedicinalesAlejandro Del Hoyo NavarreteAún no hay calificaciones
- Guia Deber 1Documento3 páginasGuia Deber 1Victor GarciaAún no hay calificaciones
- Ácido AcetilsalicílicoDocumento18 páginasÁcido Acetilsalicílicocristhian guzmanAún no hay calificaciones