Documentos de Académico
Documentos de Profesional
Documentos de Cultura
Anatomia LCA 1 PDF
Anatomia LCA 1 PDF
Cargado por
Lautaro DelaloyeTítulo original
Derechos de autor
Formatos disponibles
Compartir este documento
Compartir o incrustar documentos
¿Le pareció útil este documento?
¿Este contenido es inapropiado?
Denunciar este documentoCopyright:
Formatos disponibles
Anatomia LCA 1 PDF
Anatomia LCA 1 PDF
Cargado por
Lautaro DelaloyeCopyright:
Formatos disponibles
ACTUALIZACIONES Rev Esp Cir Osteoart 1992; 27: 33-42
Anatoma descriptiva y funcional
del ligamento cruzado anterior.
Implicaciones clnico-quirrgicas
V. SANCHIS ALFONSO y F. GOMAR SANCHO
Ctedra de Traumatologa y Ortopedia. Facultad de Medicina y Odontologa. Departamento de Ciruga.
Universidad de Valencia.
Resumen. El ligamento cruzado anterior (LCA) es una estructura anatmica vital
para la estabilidad de la rodilla y su correcta biomecnica. Su reparacin mediante
plastias exige que su tensin, direccin y punto de anclaje se aproxime en todo lo posi-
ble al LCA original. Este trabajo intenta actualizar los aspectos anatmicos y funciona-
les fundamentales para una correcta ciruga de las lesiones del LCA.
Palabras clave: Rodilla. Ligamento cruzado anterior. Roturas de ligamentos.
DESCRIPTIVE AND FUNCTIONAL ANATOMY OF THE ANTERIOR CRUCIATE LIGA-
MENT. CLINICAL AND SURGICAL IMPLICATIONS.
Summary. The anterior cruciate ligament (ACL) is a vital structure for stability of
the knee and its correct biomechanics. ACL repair by means of grafts requires that
tension, direction and attachment points resemble those of original ligament. This
work attempts to update the fundamental functional and anatomical aspects for co-
rrect surgery of ACL.
Key words: Knee. Anterior cruciate ligament. Rupture of ligaments,
INTRODUCCIN t u r a a n a t m i c a y funcional. Por otro lado las
tcnicas quirrgicas empleadas p a r a su recons-
La primera descripcin del ligamento cruza- truccin e s t n b a s a d a s en un profundo conoci-
do anterior (LCA) se debe a Galeno (1), pero no miento de su anatoma.
ser h a s t a el ao 1850 cuando Stark (2) descri-
be el primer caso de r o t u r a de este ligamento. En este trabajo p r e t e n d e m o s hacer u n a ac-
En el ao 1917, Hey-Groves (3), al que podemos tualizacin de conocimientos sobre la anatoma
considerar como padre de las ligamentoplastias, descriptiva y funcional del LCA, correlacionn-
describe la primera reconstruccin intraarticu- dola con aspectos clnicos y con la problemtica
lar del LCA; desde entonces hasta nuestros das quirrgica que plantea su reemplazo.
se suceden en la literatura ortopdica artculos
que describen tcnicas quirrgicas p a r a reem-
plazar este ligamento. Se puede afirmar que la ANATOMA MACROSCPICA
reconstruccin o reemplazo del LCA constituye
un autentico desafo y un problema todava no El LCA es u n a e s t r u c t u r a i n t r a a r t i c u l a r y
resuelto en la actualidad. La clave de toda esta extrasinovial, situada en la escotadura intercon-
problemtica es su compleja y particular estruc- dlea de la rodilla, que discurre oblicuamente,
desde su insercin a nivel de la regin antero-
medial del platillo tibial, hacia a t r s , a r r i b a y
Correspondencia: afuera, h a s t a la porcin medial del cndilo fe-
DR. VICENTE SANCHIS ALFONSO moral lateral (bien posterior y arriba, cerca de
Avda. Cardenal Benlloch, 36-23B
46021 Valencia la superficie a r t i c u l a r ) (Fig. 1). La d i s t a n c i a
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
34 REVISTA ESPAOLA DE CIRUGA OSTEARTICULAR
mxima entre las superficies internas de ambos
cndilos femorales ( a n c h u r a de la e s c o t a d u r a
intercondlea) es de 21 + 3 mm frente a los 15
3 mm en los casos de roturas inveteradas del
LCA, debido a la artrosis secundaria con osteo-
fitosis (4). Esto se t r a d u c e en la necesidad de
practicar el ensanchamiento del espacio inter-
condleo ("notch plastia") en el tratamiento qui-
rrgico de las roturas inveteradas del LCA para
evitar el a t r a p a m i e n t o ("impingement") del in-
jerto que se utilice como sustituto i n t r a a r t i c u -
lar.
El LCA adopta u n a disposicin helicoidal ca-
r a c t e r s t i c a que proporciona u n a tensin ade-
cuada del ligamento a travs de todo su rango
de m o v i m i e n t o (Fig. 2). E s t c o n s t i t u i d o por
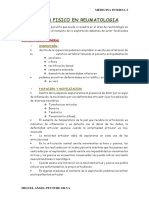
mltiples fascculos, regular y a r m n i c a m e n t e Figura 3. Imagen artroscpica del LCA que muestra su estructura
orientados (Fig. 2 y 3). Cada fibra tiene un ni- multifascicular y la gran anchura de la insercin tibial (Cortesa del
co punto de origen e insercin, no son paralelas Dr. Gastaldi).
ni t i e n e n la m i s m a l o n g i t u d y tampoco e s t n
bajo la misma tensin a lo largo de todo el arco
de flexo-extensin de la rodilla.
La longitud del ligamento es de 31 3 mm,
el espesor de 5 1 mm y la a n c h u r a 10 + 2
mm, las dos ltimas medidas en el tercio medio
del ligamento, siendo el volumen total de 2.3
4 ml (4).
El LCA, al igual que el l i g a m e n t o cruzado
posterior (LCP) y el ligamento lateral externo,
es un ligamento "cordonal" a diferencia de los
l i g a m e n t o s del complejo i n t e r n o de la rodilla
que son ligamentos "acintados" (5). Este dato es
Figura 1. Visin posterior de la escotadura intercondlea. Cndilo
femoral lateral (CL). Mun femoral del LCA resecado (asterisco).
de gran importancia prctica pues los ligamen-
Margen articular, insercin del LCA (flechas). tos cordonales, t r a s la rotura, sufren retraccin
de sus extremos y n u n c a restablecen su conti-
n u i d a d . De esto se deduce que el t r a t a m i e n t o
de u n a rotura completa del LCA debe ser la ci-
ruga (5).
El LCA est envuelto por u n a m e m b r a n a si-
novial (Fig. 2) que se hace ms evidente por de-
lante del ligamento, formando un meso, conoci-
do como ligamento mucoso, por el que discurren
los v a s o s s a n g u n e o s q u e se d i r i g e n al LCA
(Fig. 4A y 4B). E s t a e s t r u c t u r a probablemente
es un vestigio del "septum medio" que divide la
articulacin tibiofemoral en los estadios tempra-
nos del desarrollo embrionario. Cuando este ta-
bique persiste nos hallamos con la "plica sino-
vial infrapatelar". Reider y cols. (6) l l a m a n a
Figura 2. Fotografa macroscpica del LCA (1) mostrando su es-
tructura espiral y multifascicular. El LCA y el LCP estn tapizados esta e s t r u c t u r a "septum mucosum". Dicho plie-
por una cubierta sinovial comn y continua. gue sinovial est anclado proximalmente al te-
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
V. SANCHIS ALFONSO Y OTROS.- ANATOMA DESCRIPTIVA Y FUNCIONAL DEL LIGAMENTO CRUZADO ANTERIOR... 35
Figura 4. Visin anterior de la rodilla en 90 de flexin. Bolsa adi- Figura 6. Visin anterior de la escotadura intercondlea con la rodi-
posa infrapatelar de Hoffa (asterisco). A) Ligamento mucoso poco lla en flexin una vez eliminada la cubierta sinovial que envuelve
desarrollado (1). B) Ligamento mucoso muy desarrollado, plica in- ambos ligamentos cruzados. LCA (1). LCP (2). Ligamento menisco-
flapatelar (2). femoral anterior de Humphrey (3). Cuerno anterior menisco lateral
(4). Borde interno menisco lateral (flecha).
En la cara anterior del ligamento, cruzando
su tercio distal, encontramos el ligamento yu-
gal, transverso o intermeniscal anterior (Fig. 5),
interpuesto entre el ligamento y la almohadilla
grasa infrapatelar de Hoffa, que cubre la mitad
distal del ligamento. El ligamento yugal se ex-
tiende desde el cuerno anterior del menisco me-
dial al margen anterior convexo del menisco la-
teral (Fig. 5). Estas dos estructuras anatmicas,
ligamento yugal y g r a s a infrapatelar, pueden
ser la causa de que se observe una mayor proli-
feracin sinovial en el e x t r e m o p r o x i m a l del
LCA o de los injertos que lo s u s t i t u y e n (7), lo
Figura 5. Visin anterior de la escotadura intercondlea con la rodi- que provocara, como dice Alm (8) que el n-
lla en flexin. LCA (1) y LCP (2) envueltos por sinovial. Ligamento mero y calibre de las arterias, sea mayor en el
yugal (3). Fibras de insercin del cuerno anterior del menisco lateral
en la meseta tibial (4). Cuerno anterior menisco medial (5).
extremo proximal, que en el extremo distal del
ligamento. La bolsa adiposa tiene u n a gran im-
portancia prctica, pues con su rica vasculariza-
cho del espacio intercondleo, i n m e d i a t a m e n t e cin contribuye notablemente al aporte vascular
por d e l a n t e de la insercin del LCA y distal- al LCA (9). G u i l l e n y cols. (5), r e c o m i e n d a n
m e n t e comunica con la g r a s a i n f r a p a t e l a r de adosar al injerto que sustituya al LCA o al pro-
Hoffa (Fig. 4B). pio ligamento t r a s su s u t u r a la bolsa adiposa,
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
36 REVISTA ESPAOLA DE CIRUGA OSTEARTICULAR
con la idea de a u m e n t a r su vascularizacin (5). Por el c o n t r a r i o , O d e n s t e n y G i l l q u i s t (4)
Se debe pues evitar la exresis de esta grasa y en un estudio realizado sobre 33 rodillas de ca-
respetar al mximo las partes blandas en gene- dver, con u n a m e d i a de edad de 29 aos, no
ral en la ciruga del LCA, aunque ello dificulte encontraron evidencia macroscpica de subdivi-
en cierta medida la tcnica quirrgica. sin del ligamento en ninguna de ellas. Cuando
la rodilla se flexionaba a 90 el LCA se enrro-
El LCA est ntimamente relacionado con el llaba aproximadamente 90. Como resultado de
LCP, en la zona en que ambos se c r u z a n , es- sto las fibras que se o r i g i n a b a n de la p a r t e
tando cubiertos ambos ligamentos por u n a capa ms anterior del rea de insercin tibial se in-
sinovial continua (Fig. 5). El LCA se cruza en sertaban en la parte ms proximal del rea de
X con el LCP en rotacin tibial i n t e r n a adop- insercin en el cndilo femoral l a t e r a l ; por el
tando planos paralelos en rotacin externa. En c o n t r a r i o , l a s fibras q u e se o r i g i n a b a n en la
muchas ocasiones fibras del LCA se dirigen por parte ms posterior del rea de insercin tibial
detrs del LCP a la cara medial del surco inter- se i n s e r t a b a n en la p a r t e m s l a t e r a l y distal
condilar. El LCA, j u n t o con el LCP, ligamento del rea de insercin femoral. Es decir, aunque
meniscofemoral posterior de W r i s b e r g y liga- anatmicamente no exista subdivisin, funcio-
m e n t o meniscofemoral a n t e r i o r de H u m p h r e y nalmente se encontraban los dos fascculos des-
(Fig. 6), constituyen el "Pivote central" o siste- critos por Girgis y cols. (10). Appel y cols. (16)
ma ligamentoso central de la rodilla. Ahora e s t u d i a n la a n a t o m a del LCA en 50 rodillas
bien, la presencia de los ligamentos meniscofe- no encontrando tampoco separacin anatmica
morales no es constante; estando ausentes en el del ligamento en los dos fascculos (anterome-
30% de los casos (10). dial y posterolateral) cuando hacen cortes hori-
zontales del mismo; sin embargo en las disec-
A pesar de que los estudios sobre la configu- ciones longitudinales encuentran u n a configura-
racin anatmica y espacial del LCA se suce- cin cruzada de sus fascculos.
den en la l i t e r a t u r a , hoy en da todava es un
tema controvertido. Por ltimo, d e s t a c a r que observaciones ar-
troscpicas m u e s t r a n LCA con fascculos bien
Abbot y cols. (11) fueron los p r i m e r o s en individualizados y otros en los que stos no se
d e s c r i b i r u n g r u p o d e fibras a n t e r o m e d i a l e s pueden distinguir (17).
desde el punto de vista funcional, que estaban
t e n s a s en flexin. Lam (12) describe dos fasc- A la v i s t a de lo r e s e a d o en la l i t e r a t u r a
culos a los que denomina anteromedial y poste- c o n s u l t a d a , de los r e s u l t a d o s de n u e s t r a s di-
rolateral en funcin de la localizacin de la in- secciones y de nuestro material clnico artros-
sercin tibial. Girgis, Marshall y Monajem (10), cpico, podemos concluir diciendo que si bien
en un estudio sobre 20 rodillas de cadver y 24 no siempre se pueden encontrar dos fascculos
rodillas frescas, e n c u e n t r a n que el LCA e s t anatmicamente bien diferenciados si que exis-
formado por dos fascculos: fascculo anterome- t e n siempre dos porciones diferentes desde el
dial (fino) y posterolateral (porcin principal). punto de vista funcional en el LCA (Fig. 7A y
El fascculo anteromedial est formado por las 7B). D u r a n t e la extensin el LCA choca contra
fibras que se i n s e r t a n en la p a r t e m s proxi- el techo de la escotadura intercondlea lo cual
mal de la insercin femoral a la ms anterior y limita u n a mayor extensin. A medida que va-
m e d i a l de la i n s e r c i n t i b i a l . L a s fibras que mos incrementando los grados de flexin de la
van de la porcin ms distal de la insercin fe- rodilla los dos fascculos se e n r r o l l a n r o t a n d o
moral y se insertan en la porcin posterolateral l a s fibras p o s t e r o l a t e r a l e s por debajo de l a s
del anclaje tibial constituyen el fascculo pos- a n t e r o m e d i a l e s . El ligamento pierde su forma
t e r o l a t e r a l . N a v a r r o y cols. (13) t a m b i n en- de abanico, que p r e s e n t a con la extensin de
c o n t r a r o n en t o d o s los casos e s t u d i a d o s por la rodilla, y va a s u m i e n d o u n a forma de cor-
ellos (54 rodillas procedentes de miembros am- dn r e d o n d o y e n r r o l l a d o . V a n Dick (18) de-
putados) dos fascculos bien diferenciados ana- mostr que las fibras del LCA no son p a r a l e -
tmica y funcionalmente. Estos dos fascculos l a s e n l a e x t e n s i n sino q u e p r e s e n t a n u n a
tambin son descritos por Minguet (7). En 1979 t o r s i n e x t e r n a de 46. C u a n d o la rodilla se
Norwood y Cross (14) describen un tercer fasc- flexiona a 90 el ngulo de torsin se incre-
culo m s pequeo denominado fascculo inter- m e n t a a 105, lo que pone de m a n i f i e s t o ese
medio, hallazgo t a m b i n encontrado en el ao enrrollamiento progresivo que el ligamento su-
1985 por Dawkins y Amis (15). fre con la flexin de la rodilla.
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
V. SANCHIS ALFONSO Y OTROS.- ANATOMA DESCRIPTIVA Y FUNCIONAL DEL LIGAMENTO CRUZADO ANTERIOR... 37
U n a vez vista la configuracin y orientacin Significado funcional de los puntos de
espacial del LCA, vamos a centrarnos en el es- anclaje. Concepto de "isometricidad",
tudio de los puntos de anclaje y su significado realidad o fantasa?
funcional.
Actualmente se da gran importancia al con-
Anclaje tibial cepto de "isometricidad", pero no se t r a t a de un
trmino nuevo. En el ao 1942 Blair (22) suge-
E l LCA s e i n s e r t a e n u n a fosita s i t u a d a ra la eleccin de un punto de anclaje en el f-
a n t e r o l a t e r a l m e n t e respecto a la espina tibial m u r que no modificara la distancia respecto al
anterior. P a s a por debajo del ligamento yugal punto tibial a lo largo de todo el arco de flexo-
y u n o s pocos fascculos se e n t r e m e z c l a n con e x t e n s i n de la rodilla. E s t e a u t o r c i t a como
el cuerno a n t e r i o r del menisco l a t e r a l en to- fuente un trabajo de T e s t u t de 1911 (23). As
dos los casos (Fig. 5) y con el c u e r n o p o s t e - mismo Blair (22), refirindose al "injerto", dice
rior del menisco l a t e r a l en el 20% de casos. que en esta situacin ste tendr el mismo gra-
El LCA t i e n e f i b r a s a n c l a d a s en la b a s e de do de tensin a lo largo de todo el recorrido de
la e s p i n a tibial a n t e r i o r pero no en el v r t i - flexo-extensin de la rodilla. De forma implcita
ce. estaba expresando que la "isometricidad" en el
anclaje supone u n a "isotonicidad" del implante,
El anclaje tibial es m s ancho y fuerte que con lo que s t e e s t a r sometido a un " s t r e s s
el anclaje f e m o r a l . E s t o p u e d e e x p l i c a r que t e n s i l " uniforme a lo largo de todo el arco de
sea m s frecuente la desinsercin a nivel del m o v i m i e n t o de flexo-extensin de la r o d i l l a .
a n c l a j e f e m o r a l q u e t i b i a l (19). A s , I n s a l l Tengamos en c u e n t a que el "stress tensil" es
(20) e n c u e n t r a u n a frecuencia del 18% de ro- necesario p a r a la morfognesis, remodelacin y
t u r a s completas a nivel de la insercin femo- m a d u r a c i n de la colgena (24,25,26). A h o r a
r a l frente al 2% de r o t u r a s a nivel de la in- bien, no hay actualmente ningn autor que nos
sercin tibial, provocando s t a s l t i m a s avul- pueda decir que tensin concreta debe tener el
sin sea. implante p a r a asegurar un buen futuro al mis-
mo. La mayora de los autores solo nos hablan
P a r a Odensten y Gillquist (4) el rea de in- de una "tensin firme" (27,28,29).
sercin tibial es oval, con su eje mayor orienta-
do en sentido antero-posterior. Su longitud es P a r a conseguir la "isometricidad", es condi-
de 17 + 3 mm y su a n c h u r a de 11 2 mm. El cin necesaria la correcta eleccin de los puntos
punto central de la insercin tibial esta locali- de a n c l a j e ( f e m o r a l y t i b i a l ) , lo c u a l ya e r a
zado a 7 1 mm del plano del borde anterior puesto de manifiesto por Palmer (30).
de la superficie articular del cndilo tibial me-
dial y a 23 + 4 mm de la unin meniscocapsu- La eleccin del punto de anclaje femoral es
lar anterior en el cndilo tibial medial. crtica a la hora de realizar u n a reconstruccin
isomtrica del LCA, pues el punto femoral es el
Anclaje femoral determinante primario de la "isometricidad"
(31). Por otro lado tambin se t r a t a de un tema
El LCA se i n s e r t a en u n a fosita s i t u a d a en controvertido, habindose descrito varios puntos
la p a r t e posterior de la superficie m e d i a l del de anclaje t r a n s s e o s o a n a t m i c o s (32) y un
cndilo femoral lateral. anclaje e x t r a - a n a t m i c o ("over-the-top") (33).
Nosotros siguiendo las ideas de Clancy y cols.
P a r a nosotros, al igual que p a r a otros auto- (34) elegimos en n u e s t r o s pacientes un p u n t o
res (10,21), el rea de anclaje femoral tiene la situado 5 mm posterosuperior al centro de in-
forma de un segmento de crculo con su borde sercin anatmica normal del LCA. De esta for-
anterior recto y el posterior convexo, siendo es- ma este punto isomtrico se localiza en la parte
te ltimo paralelo al margen articular posterior m s posterior de la lnea de B l u m e n s a a t , que
del cndilo femoral l a t e r a l (Fig. 8A y 8B). Por es la lnea que se puede proyectar en u n a ra-
el contrario Odensten y Gillquist (4) encuentran diografa de perfil de la rodilla sobre el surco
que el rea de insercin femoral es oval, con un intercondleo. La reinsercin femoral del LCA
d i m e t r o mayor de 18 2 mm y un dimetro se debe realizar con la rodilla flexionada 120
menor de 11 2 mm. El ngulo entre el dime- en un p u n t o lo m s posterior y abajo posible
tro mayor del valo y el eje de la difisis femo- del cndilo externo. Un e m p l a z a m i e n t o dema-
ral es de 26 + 7. siado anterior del tnel femoral conduce a u n a
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
38 REVISTA ESPAOLA DE CIRUGA OSTEARTICULAR
Figura 7. Visin medial de la rodilla una vez eliminado el cndilo femoral medial. Cambio en la forma y tensin de los componentes del
LCA con la flexin y extensin. A) Rodilla en extensin. B) Rodilla en flexin, fascculo anteromedial tenso (flechas).
tensin y elongacin excesiva del injerto en fle- una rotura del implante (35). Si los tneles seos
xin, debido a la o r i e n t a c i n v e r t i c a l del im- tibial y femoral se perforan en los centros anat-
p l a n t e , lo cual s u p o n d r u n a restriccin de la micos originales, las fijaciones del implante liga-
flexin y a la larga la rotura del implante (35). mentoso e s t a r n demasiado cerca y tendremos
problemas de dficit de extensin y flexin de la
Un estudio comparativo del efecto de la inser- rodilla, porque el nuevo ligamento ser demasia-
cin femoral y tibial en la isometra muestra que do corto.
la insercin femoral es de m a y o r i m p o r t a n c i a
que la insercin tibial (36). No obstante la inser- A h o r a bien, no existe un p u n t o isomtrico
cin tibial es fundamental para que la longitud y nico o absoluto. Las discrepancias de los hallaz-
orientacin espacial del injerto en la articulacin gos publicados en la l i t e r a t u r a son debidas no
sea correcta. Nosotros elegimos, al igual que slo a diferencias en las condiciones experimen-
Clancy y cols. (34), un punto situado 5 mm ante- tales sino tambin al hecho de que cada rodilla
romedial al centro anatmico del LCA, por de- tiene sus propios puntos isomtricos (37). Las ro-
t r s del cuerno anterior del menisco medial. Se dillas de cada persona, por otro lado, tambin di-
debe evitar realizar el tnel tibial demasiado an- fieren en las dimensiones seas y en la resisten-
teriormente pues esto supondra u n a limitacin cia y grosor de sus ligamentos cruzados. De esto
en la extensin de la rodilla, con una predisposi- se deduce que la isometricidad debe ser evaluada
cin al atrapamiento del injerto contra el techo antes de perforar los tneles seos. Un emplaza-
de la escotadura intercondlea (35). P a r a evitar miento isomtrico es definido como aquel en que
el "impingement" se recomienda, en estos casos, la distancia entre la insercin femoral y tibial no
la realizacin de la condiloplastia ("notchplasty"). cambia m s de 1.5-2 mm cuando la rodilla es
Si el punto de anclaje tibial es demasiado poste- flexionada de 0 a 90 (36,37) .
rior se producir un incremento de la distancia
entre los puntos de anclaje femoral y tibial cuan- Desde el punto de vista anatmico el LCA no
do la rodilla se extiende, lo cual se traducir en es "isomtrico" en el sentido estricto de la palabra
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
V. SANCHIS ALFONSO Y OTROS.- ANATOMA DESCRIPTIVA Y FUNCIONAL DEL LIGAMENTO CRUZADO ANTERIOR... 39
Figura 8. Insercin femoral del LCA (rojo). A) Visin medial una vez eliminado el cndilo femoral medial. Punto isomtrico femoral (asteris-
co). B) Visin posterior.
(38). Por otro lado, es incorrecto hablar de "pun- Desde nuestro punto de vista la mejor forma
to isomtrico", debindose hablar de "rea isom- de aproximarse a la realidad, cuando nos plante-
trica" (31). Adems la superficie del "rea isom- amos el reemplazo del LCA lesionado, es utilizar
trica" disminuye conforme aumenta la flexin de la tcnica del doble fascculo (39,40), tcnica que
la rodilla, motivo por el cual la evaluacin pero- nosotros estamos empleando en la actualidad.
peratoria de la tensin del implante debe ser re- Con esta tcnica lo que hacemos es combinar el
alizada a lo largo de todo el arco de flexo-exten- anclaje transseo femoral con uno over-the-top
sin de la rodilla (31). Si tenemos en cuenta que con lo que conseguimos estabilidad anteroposte-
el "rea isomtrica" es m s p e q u e a que los rior de la rodilla tanto a 90 de flexin de la ro-
sustitutos que normalmente se emplean para re- dilla como a 20.
emplazar al LCA lesionado se comprender que
realmente alcanzar la isometricidad es un objeti- ANATOMA FUNCIONAL
vo utpico (31).
Anatoma artroscpica dinmica
Se puede concluir diciendo que el concepto
de isometricidad es ms bien un recurso quirr- La inspeccin artroscpica del LCA en varias
gico p a r a aproximarnos a la realidad del papel posiciones de flexin de la rodilla ha incrementa-
que d e s e m p e a el LCA en la cinemtica de la do considerablemente los conocimientos sobre su
rodilla que una realidad anatmica. Con ello per- funcin.
seguimos un doble objetivo: a) Proteccin del im-
plante contra una excesiva elongacin y stress, lo En el paciente sometido a anestesia general
que se traducir en u n a "sobrevivencia" prolon- Johnson (17) estudia la laxitud del LCA entre
gada del implante y b) Freno contra el cajn an- 90 de flexin y la e x t e n s i n c o m p l e t a .
terior femoro-tibial durante la flexo-extensin de Encuentra que entre los 90 y 45 el ligamento
la rodilla. se e n c u e n t r a laxo. M s all de e s t e p u n t o la
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
40 REVISTA ESPAOLA DE CIRUGA OSTEARTICULAR
tensin del ligamento se i n c r e m e n t a g r a d u a l - b) La seccin completa del LCA conduce a una
m e n t e a m e d i d a que a u m e n t a la extensin de inestabilidad rotacional evidente (Maniobra del
la rodilla. Pivot-Shift positiva). La seccin aislada de los fasc-
culos no causa inestabilidad rotacional detectable
Si el e s t u d i o se h a c e con el p a c i e n t e bajo clnicamente. El LCA es un estabilizador primario
anestesia local es posible su cooperacin , de tal contra la inestabilidad rotatoria anterolateral (42).
forma que podremos evaluar el efecto de la con-
traccin del cudriceps en la tensin del LCA. c) Los dos fascculos se t e n s a n al m x i m o
La t e n s i n del LCA se i n c r e m e n t a cuando se cuando la rodilla extendida se rota internamente.
contrae el cudriceps contra resistencia e n t r e Si tenemos en cuenta que la extensin de la rodi-
los 45 y 0 o . Esto tiene una gran relevancia cl- lla tensa al mximo el fascculo posterolateral se
nica en el proceso de rehabilitacin tras ciruga explica que un mecanismo de hiperextensin ms
del LCA. Cualquier contraccin del cudriceps rotacin interna sea causa de rotura aislada del
con la rodilla en 45 de flexin o menos t e n s a LCA (43) , lo cual ha sido comprobado clnica-
el LCA. La rehabilitacin consistir idealmente mente. Tambin la hiperextensin aislada ("chut
en ejercicios i s o m t r i c o s en 45 de flexin o al vaco") es causa de rotura del LCA.
ms junto con ejercicios de isquiotibiales (anta-
gonistas del cudriceps). d) La rotura del LCA incrementa la hiperex-
tensin de la rodilla, siendo el papel del fasc-
De estos estudios Johnson (17) concluye que culo posterolateral como barrera contra la hipe-
el LCA no es funcionalmente isomtrico, con lo rextensin ms importante que el del fascculo
cual se vuelve a cuestionar el concepto de iso- anteromedial.
metricidad.
El hecho de que segn la posicin de flexo-
Estudios post-mortem extensin un fascculo est tenso y el otro rela-
jado, explicara la existencia de r o t u r a s parcia-
Girgis y cols. (10) demostraron que la por- les del l i g a m e n t o . A d e m s , en funcin de los
cin a n t e r o m e d i a l e s t t e n s a e n flexin, fascculos lesionados la exploracin clnica va-
m i e n t r a s que la p o s t e r o l a t e r a l e s t t e n s a en r i a r . Si solamente es positivo uno de los dos
e x t e n s i n . F u r m a n y cols. (41) h i c i e r o n un signos (cajn anterior o test de Lachman) debe-
e s t u d i o f u n c i o n a l del LCA u t i l i z a n d o p a r a remos p e n s a r en u n a r o t u r a parcial del LCA.
ello 40 rodillas de cadver fresco h u m a n o ; su Por ejemplo, un test de Lachman positivo y un
objetivo e r a e s t u d i a r el p a p e l que d e s e m p e - cajn anterior negativo implica u n a r o t u r a del
a b a n c a d a u n o d e los fascculos e n e x t e n - fascculo posterolateral del LCA.
sin, 45 y 90 de flexin, as como la r e s i s -
t e n c i a que ofrece el LCA a la r o t a c i n e hi- El m o v i m i e n t o de flexin de la r o d i l l a es
p e r e x t e n s i n de la rodilla. Obtuvieron los si- mixto: de r o d a d u r a y de deslizamiento antero-
guientes resultados: posterior de la tibia sobre el fmur, siendo la
relacin normal de ambos movimientos de 1:2
a) El signo del cajn anterior, despus de la al principio de la flexin y de 1:4 con la flexin
seccin del fascculo posterolateral, es positivo completa (44). Con la rotura del LCA se altera
con la r o d i l l a en e x t e n s i n ( M a n i o b r a de esta relacin normal, predominando la primera
Lachman positiva) y negativo con la rodilla en d u r a n t e los primeros grados de flexin , lo que
flexin (Cajn anterior negativo), puesto que en implica u n a subluxacin anterior de la tibia lo
flexin est tenso el fascculo anteromedial. En cual unido al mayor radio de curvatura del cn-
flexin el fascculo anteromedial constituye u n a dilo femoral lateral hace que la tibia rote inter-
barrera de primer orden para el desplazamiento n a m e n t e . El cudriceps a c t a f a v o r e c i e n d o la
anterior de la tibia respecto del fmur. Si se sec- subluxacin anterior, mientras que la fascia la-
ciona el fascculo anteromedial, el posterolateral ta acta favoreciendo la luxacin en extensin y
que permanece intacto se tensa indicando que es reducindola en flexin. En estos principios bio-
u n a barrera de segundo orden para el signo del mecnicos se basa el test del pivot-shift. La re-
cajn anterior en posicin de flexin. Si secciona- p e r c u s i n de e s t e "fenmeno del r e s a l t e " del
mos por completo el LCA el signo del cajn ante- compartimento externo sobre el interno, se tra-
rior es marcadamente positivo en todas las posi- duce progresivamente por la lesin del cuerno
ciones (Maniobra de Lachman positiva y Cajn p o s t e r i o r del menisco i n t e r n o , la l a x i t u d del
anterior positivo). punto del ngulo postero-interno (PAPI) y por
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
V. SANCHIS ALFONSO Y OTROS.- ANATOMA DESCRIPTIVA Y FUNCIONAL DEL LIGAMENTO CRUZADO ANTERIOR... 41
ltimo la aparicin de lesiones del cartlago ar- n e s del m e n i s c o m e d i a l (49) e n l a s r o d i l l a s
ticular que abocar irremediablemente en la ar- LCA-deficientes.
trosis uni, bi o tricompartimental de la rodilla.
En la historia natural de la rotura completa del Adems como funciones secundarias tendra
LCA encuentra su mayor justificacin el t r a t a - las s i g u i e n t e s : r e s i s t e n c i a frente al varo y al
miento quirrgico de estas lesiones. valgo y g u a de la t i b i a en el m o v i m i e n t o de
autoatornillamiento final de la extensin de la
Podemos concluir diciendo que el LCA ac- rodilla. Por tensarse en la hiperextensin de ro-
t a como b a r r e r a frente a la t r a s l a c i n a n t e - dilla, se t r a t a de un a n t a g o n i s t a del msculo
rior de la tibia respecto al fmur, frente a la cuadrceps, por lo que en las s u t u r a s o sustitu-
hiperextensin y frente a la excesiva rotacin ciones de e s t e l i g a m e n t o se debe r e t r a s a r al
i n t e r n a . B u t l e r y cols. (45) d e m o s t r a r o n que a mximo en ganar la extensin de rodilla.
90 de flexin el LCA proporciona el 8 5 . 1 %
1.9% de la fuerza contra la traslacin anterior H e m o s visto p u e s como t r a s la l e s i n del
de la tibia respecto al fmur. A 30 de flexin LCA la cinemtica de la rodilla se altera, por lo
este porcentaje se incrementa ligeramente. que la reconstruccin del LCA debe tener efec-
Ahora bien, este efecto de b a r r e r a no es de la tos potencialmente beneficiosos, aunque an es-
misma intensidad en todos los ngulos de fle- t por demostrar si dicha reconstruccin es ca-
xo-extensin de la rodilla. As, la t r a s l a c i n paz de r e s t a u r a r por completo la biomecnica
a n t e r i o r de la tibia respecto al fmur es ma- de una rodilla LCA deficiente y si realmente es-
yor cerca de los 30 de flexin (46) y e s t a es ta reconstruccin tiene un efecto protector con-
la r a z n por la que n o s o t r o s , al igual que t r a ulteriores cambios artrsicos (50). Nosotros
o t r o s a u t o r e s (47), p r e f e r i m o s t e n s a r e l im- s u s c r i b i m o s las i d e a s de I v a r P a l m e r (30) el
p l a n t e a 30 de flexin de la rodilla. T r a s la cual en el ao 1938 ya indicaba que "incluso en
seccin completa del LCA el menisco m e d i a l el mejor de los casos, no se p u e d e c o n s e g u i r
es u n a b a r r e r a significativa frente a la trasla- una restitutio ad integrum tras realizar la plas-
cin a n t e r i o r d e l a t i b i a r e s p e c t o a l f m u r tia i n t r a a r t i c u l a r " , lo cual no quita mritos al
(48). Esto explica la a l t a incidencia de lesio- efecto beneficioso que tiene la ciruga.
Bibliografa
1. G a l e n C. On t h e usefulness of t h e p a r t s of t h e body. May, MT ( t r a n s ) . I t h a c a , Cornell U n i v e r s i t y P r e s s , 1968; pp
22,90,151,197,550.
2. Stark J. Two cases of rupture of the crucial ligament of the knee-joint. Edinb Surg 1850; 74: 267-71.
3. Hey-Groves EW. Operation for the repair of the crucial ligaments. Lancet 1917; 2: 674-5.
4. O d e n s t e i n M, Gillquist J. Functional anatomy of the anterior cruciate ligament and a rationale for reconstruction. J.
Bone Joint Surg 1985; 67-A: 257-62.
5. Guillen Garca P, J i m n e z Collado J, Concejero Lpez V, Abad Morenilla JM. Anatoma quirrgica de la rodilla.
Rev Ortop Traum 1984; 28: 251-66.
6. R e i d e r B, Marshall JL, Warren RF. Persistent vertical septum in t h e h u m a n knee joint. J. Bone Joint Surg 1981;
63: 1185-7.
7. M i n g u e t B a i x a u l i J E . Aloinjertos y Autoinjertos de ligamento cruzado anterior de la rodilla: Estudio experimental de
su revascularizacin e histologa. Sevilla: Universidad de Sevilla, 1990; Tesis Doctoral.
8. Aim A, Stromberg B. Vascular anatomy of the patellar and cruciate ligaments: a microangiographic and histologic in-
vestigation in the dog. Acta Chir Scand (supl). 1974; 445: 25-35.
9. Arnoczky SP. The vascularity of the anterior cruciate ligament and associated structures. Its role in repair and recons-
truction. En: Jackson, DW y Drez, D, eds: The anterior cruciate deficient knee. New concepts in ligament repair. St
Louis: C.V. Mosby Company. 1987; 27-54.
10. Girgis FG, Marshall JL, Al Monajem ARS. The Cruciate Ligaments of the Knee Joint. Anatomical, Functional and
Experimental Analysis. Clin Orthop 106; 1975: 216-31.
11. A b b o t t LC, S a u n d e r s J B , B o s t FC, A n d e r s o n CE. Injuries to the ligaments of t h e knee joint. J Bone J o i n t Surg
1944; 26: 503-21.
12. Lam S J S . Reconstruction of the anterior cruciate ligament using the Jones procedure and its Guy's Hospital modifica-
tion. J Bone Joint Surg 1968; 50A: 1213-24.
13. Navarro Quilis A. Inestabilidad ligamentosa de la rodilla. Ponencia Oficial del XXI Congreso de la Sociedad Espaola
de Ciruga Ortopdica y Traumatologa (S.E.C.O.T.). VI Congreso Hispano-Argentino de Traumatologa y Ortopedia.
Reunin Hispano-Mejicana de Traumatologa y Ortopedia. Reunin de la Sociedad Latino-Americana de Ortopedia y
Traumatologa (S.L.A.O. T.). Sevilla 14-18 de Abril de 1983.
14. N o r w o o d LA, Cross MJ. Anterior cruciate ligament: functional anatomy of its bundles in rotatory instabilities. Am J
Sports Med 1979; 7: 23-6.
VOLUMEN 27; N2 157; ENERO-FEBRERO, 1992
42 REVISTA ESPAOLA DE CIRUGA OSTEARTICULAR
15. D a w k i n s GPC, A m i s AA. A functional study of the structure of t h e anterior cruciate ligament, related to knee stabi-
lity, injury mechanisms and prosthetic ligament reconstructions. J Bone Joint Surg 1985; 67: 844.
16. A p p e l M, G r a d i n g e r R, P i e p e r B, H i p p E. The anatomy of the h u m a n cruciate ligaments. Third Congress of t h e
European Society of Knee Surgery and Arthroscopy. Amsterdam, The Netherlands. May 16-20, 1988. (Abstract Book).
17. J o h n s o n LL. Arthroscopic Surgery. The CV Mosby Company. 1986.
18. Van Dijk R. The behaviour of the cruciate ligaments of the h u m a n knee. Niederlande: Universitat Nijmegen. 1983.
19. M a i n WK , S c o t t WN. Knee Anatomy. En: Scott WN, ed: Ligament and extensor m e c h a n i s m injuries of t h e k n e e .
Diagnosis and treatment. St. Louis:Mosby Year Book. 1991: 13-32.
20. Insall JM. Ciruga de la rodilla.Buenos Aires: Editorial Mdica Panamericana, 1984.
21. Arnoczky SP. Anatomy of the anterior cruciate ligament. Clin Orthop 1983; 172:19-25.
22. Blair HC. A simple operation for stabilization of the knee joint. Surg Gynecol Obstet 1942; 74: 855-9.
23. Testut L, ed. Traite d'anatomie humaine. 6th ed., book I. Paris: O. Doin & Sons, 1911.
24. K r i p p a e h n e WW, H u n t TK, J a c k s o n D S , D u n p h y J E . Studies on t h e effect of stress on t r a s p l a n t s of autologous
and homologous connective tissue. Am J Surg 1962; 104: 267-72.
25. Klein L, L u n s e t h PA, A a d a l e n RJ. Comparison of functional and non-functional tendon grafts. Isotopic measurement
of collagen turnover and mass. J Bone Joint Surg 1972; 54A: 1745-53.
26. Harris AK, Stopak D, Wild P. Fibroblast traction as a mechanism for collagen morphogenesis. Nature 1981; 290: 249-51.
27. Marshall JL, Warren RF, Wickiewicz TL, R e i d e r B. The anterior cruciate ligament: a technique of repair and re-
construction. Clin Orthop 1979; 143: 97-106.
28. I n s a l l J J , J o s e p h DM, A g l i e t t i P, C a m p b e l l R D . Bone-block iliotibial-band transfer for anterior cruciate insuffi-
ciency. J Bone Joint Surg 1981; 63A: 560-9.
29. N o y e s FR, Butler DL, P a u l o s LE, Grood ES. Intra-articular cruciate reconstruction. I: Perspectives on graft strength,
vascularization and inmediate motion after replacement. Clin Orthop 1983; 172: 71-7.
30. P a l m e r I. On the injuries to the ligaments of the knee joint. Acta Chir Scand (Suppl) 1938; 53.
31. H e f z y MS, G r o o d E S , N o y e s F. Factors affecting the region of most isometric femoral a t t a c h m e n t s , p a r t II. Am J
Sports Med 1989; 17: 208-16.
32. F u s s FK. Optimal replacement of the cruciate ligaments from the functional-anatomical point of view. Acta Anat 1991;
140: 260-8.
33. Mac Intosh D. The anterior cruciate ligament: over the top repair. J Bone Joint Surg 1974; 56B: 591.
34. Clancy WG, N e l s o n DA, R e i d e r B, N a r e c h a n i a RG. Anterior cruciate ligament reconstruction using one-third of the
patelar ligament augmented by extra-articular tendon transfers. J Bone Joint Surg 1982; 64A: 352-9.
35. D a n i e l DM. Principles of k n e e l i g a m e n t s u r g e r y . En: Daniel DM, Akeson W, O ' C o n n o r J (eds). Knee l i g a m e n t s .
Structure, function, injury and repair. New York: Raven Press, 1990: 11-29.
36. B r a d l e y J, F i t z P a t r i c k D, D a n i e l D, Shercliff T, O'Connor J. Orientation of the cruciate ligament in the sagittal
plane. J Bone Joint Surg 1988; 70B: 94-9.
37. Strobel M, Stedtfeld HW. Diagnostic evaluation of the knee. Springer-Verlag, 1990.
38. Amis AA, D a w k i n s GPC. Functional anatomy of the anterior cruciate ligament. J Bone Joint Surg 1991; 73: 260-7.
39. Radford WJR, A m i s AA. Biomechanical properties of a double prosthetic ligament in the anterior cruciate deficient
knee. J Bone Joint Surg 1990; 72B: 1038-43.
40. Zaricznyj B. Reconstruction of the anterior cruciate ligament of the knee using a doubled tendon graft. Clin Orthop
1987; 220: 162-75.
41. F u r m a n W, Marshall JL, Girgis FG. The Anterior Cruciate Ligament. A Functional Analysis Based on Postmortem
Studies. J Bone Joint Surg 1976; 58A: 179-85.
42. L i p k e JM, J a n e c k i C J. The role of incompetence of the anterior cruciate and lateral ligaments in anterolateral and
anteromedial instability. J Bone Joint Surg 1981; 63A: 954-60.
43. Wang J B , R u b i n RM, Marshall JL. A mechanism of isolated anterior cruciate ligament rupture. Case report. J Bone
Joint Surg 1975; 57A: 411-3.
44. B o n n a r e n s FO, Drez D J r . Clinical examination of t h e knee for anterior cruciate ligament laxity. En: Jackson DW,
Drez, D eds. The anterior cruciate deficient knee. St. Louis: Mosby,1987: 72-89.
45. B u t l e r DL, N o y e s FR, G r o o d E S . Ligamentous r e s t r a i n t s to anterior-posterior drawer in t h e h u m a n knee. J Bone
Joint Surg 1980; 62A: 259-70.
46. N o y e s FR, G r o o d E S . Classification of ligament injuries. En: AAOS Instructional Course Lectures, ed. by Griffin P,
American Academy of Orthopaedic Surgeons, Park Ridge, IL, 1987: 185-200.
47. B y l s k i - A u s t r o w DI, Grood ES, Hefzy MS, H o l d e n J P , B u t l e r DL. Anterior cruciate ligament replacements: A me-
chanical study of femoral a t t a c h m e n t location, flexion angle at tensioning and initial tension. J Orthop Res 1990; 8:
522-31.
48. L e v y IM, Torzilli PA, W a r r e n RF. The effect of medial meniscectomy on anterior-posterior motion of t h e knee. J
Bone Joint Surg. 1982, 64A: 883-8.
49. Kornblatt I, Warren RF, Wickiewicz TL. Long-term follow-up of anterior cruciate ligament reconstruction using the
cuadrceps tendon substitution for chronic anterior cruciate ligament insufficiency. Am J Sports Med. 1988; 16: 444-8.
50. F i s c h e r SP, Ferkel RD. Biomechanics of the knee. En: Friedman MJ, Ferkel RD: Prosthetic ligament reconstruction of
the knee. Philadelphia: WB Saunders Company, 1988: 3-9
VOLUMEN 27; N 157; ENERO-FEBRERO, 1992
También podría gustarte
- PLEXO BRAQUIAL CuadroDocumento1 páginaPLEXO BRAQUIAL CuadroGeneración 2011Aún no hay calificaciones
- Artrosis de RodillaDocumento30 páginasArtrosis de RodillaFernanda SanchezAún no hay calificaciones
- Inclusión de La Flexibilidad en El Entrenamiento Del FisicoculturismoDocumento12 páginasInclusión de La Flexibilidad en El Entrenamiento Del FisicoculturismoJENNY LIZETH MARTINEZ ROJAS100% (1)
- Ritmo Idioventricular AceleradoDocumento4 páginasRitmo Idioventricular AceleradoRicardo QuinteroAún no hay calificaciones
- Taquicardia SinusalDocumento4 páginasTaquicardia SinusalRicardo QuinteroAún no hay calificaciones
- CA Pulmon IntramedDocumento21 páginasCA Pulmon IntramedPedro OrbeAún no hay calificaciones
- Extrasistoles AuricularesDocumento5 páginasExtrasistoles AuricularesRicardo QuinteroAún no hay calificaciones
- Bradicardia SinusalDocumento3 páginasBradicardia SinusalRicardo QuinteroAún no hay calificaciones
- ClindamicinaDocumento5 páginasClindamicinaRicardo Quintero100% (1)
- BazoDocumento15 páginasBazoEdr MendozaAún no hay calificaciones
- Sego 05Documento178 páginasSego 05MAPA0802Aún no hay calificaciones
- Parte 06Documento120 páginasParte 06Ricardo QuinteroAún no hay calificaciones
- Sego 10Documento199 páginasSego 10rolomaxitoAún no hay calificaciones
- Partos en Presentacion de CaraDocumento2 páginasPartos en Presentacion de CaraRicardo QuinteroAún no hay calificaciones
- Revista SVCOT 41-2 CompletaTRAUMATOLOGIADocumento85 páginasRevista SVCOT 41-2 CompletaTRAUMATOLOGIARicardo QuinteroAún no hay calificaciones
- Fases de Consolidacion OseaDocumento1 páginaFases de Consolidacion OseaRicardo QuinteroAún no hay calificaciones
- ClapDocumento298 páginasClapRicardo QuinteroAún no hay calificaciones
- Power Lesiones TendinosasDocumento9 páginasPower Lesiones TendinosasCata AcevedoAún no hay calificaciones
- Cinesiterapia y MecanoterapiaDocumento3 páginasCinesiterapia y Mecanoterapiaisabela camargoAún no hay calificaciones
- Cinetica y Cinematica EscapularDocumento54 páginasCinetica y Cinematica Escapularkineunab97% (30)
- Sistema ÓseoDocumento4 páginasSistema ÓseoMARIA PAULAAún no hay calificaciones
- Carrie M Hall Ejercicio Terapeutico Recuperacion FuncionalDocumento5 páginasCarrie M Hall Ejercicio Terapeutico Recuperacion FuncionalLuis Alberto Aparicio FloresAún no hay calificaciones
- Resumen Biofisica MuscularDocumento2 páginasResumen Biofisica MuscularYizeth Tellez VargasAún no hay calificaciones
- LABHISTO-14 - Tejido Muscular - 2021 DMOR-0011Documento9 páginasLABHISTO-14 - Tejido Muscular - 2021 DMOR-0011sofiaAún no hay calificaciones
- Capitulo 5Documento48 páginasCapitulo 5Brandon Alexis ValenciaAún no hay calificaciones
- Semiologia de Miembros SuperioresDocumento30 páginasSemiologia de Miembros SuperioresValeria Agualimpia Murillo100% (1)
- Tobillo BiomecanicaDocumento30 páginasTobillo BiomecanicaChristian B. Centeno100% (1)
- HC EsguinceDocumento8 páginasHC EsguinceHeidy SarmientoAún no hay calificaciones
- Examen Fisico en ReumatologiaDocumento8 páginasExamen Fisico en ReumatologiaMiguel Ángel Pfuture SilvaAún no hay calificaciones
- RIZARTROSISDocumento8 páginasRIZARTROSISBhima PedrerosAún no hay calificaciones
- Las Articulaciones Ciencias SatyDocumento4 páginasLas Articulaciones Ciencias SatyMultiservicios E&EAún no hay calificaciones
- Expo ContracciónDocumento19 páginasExpo ContracciónOrtega Maldonado OlafAún no hay calificaciones
- Biomecanica de Rodilla y EvaluacionDocumento28 páginasBiomecanica de Rodilla y EvaluacionJesus Calderon ValverdeAún no hay calificaciones
- Musculos Del CuerpoDocumento42 páginasMusculos Del CuerpoEtmer BuendiaAún no hay calificaciones
- FNP ArticuloDocumento14 páginasFNP ArticuloStaranFisioterapiaCoordinadorAún no hay calificaciones
- GAP Nro. 6 SEPTIMODocumento12 páginasGAP Nro. 6 SEPTIMOdarlenisAún no hay calificaciones
- Guia Practica de Los 3 Basicos NujbzkDocumento77 páginasGuia Practica de Los 3 Basicos NujbzkDennis Pérez100% (1)
- 3-CFC - ArtrologíaDocumento36 páginas3-CFC - ArtrologíaVivian DSS100% (1)
- 4 - Generalidades de MiologiaDocumento8 páginas4 - Generalidades de MiologiaFernanda de Melo100% (4)
- Articulaciones MMSS y MMII.Documento49 páginasArticulaciones MMSS y MMII.Jorge O. Suárez Sánchez100% (1)
- Sobrecarga PosturalDocumento36 páginasSobrecarga PosturalVoyager1856Aún no hay calificaciones
- Morfometría de La Cavidad Glenoidea de La Escapula.: Gaceta Médica de Caracas January 2015Documento6 páginasMorfometría de La Cavidad Glenoidea de La Escapula.: Gaceta Médica de Caracas January 2015Marisha CastroAún no hay calificaciones
- EntrenamientoDocumento3 páginasEntrenamientocgarriga1Aún no hay calificaciones
- Aparato LocomotorDocumento7 páginasAparato LocomotorAlexis Arias HuaytoAún no hay calificaciones