También podría gustarte
- VEE.006 (03-20) 2 Solicitud Credisocial Productivo Persona JurídicaDocumento3 páginasVEE.006 (03-20) 2 Solicitud Credisocial Productivo Persona JurídicaNORSAID NORAIMA Y SAIDAún no hay calificaciones
- Solicitud crédito empresaDocumento5 páginasSolicitud crédito empresaJose Gramajo de Leon0% (1)
- 02-193 Inscripción Proveedores JuridicaDocumento2 páginas02-193 Inscripción Proveedores JuridicaCarlos eduardo garcia murilloAún no hay calificaciones
- Fianza AduanalDocumento2 páginasFianza AduanalSherly Lineth RamírezAún no hay calificaciones
- Form 720Documento7 páginasForm 720Andrea Urdininea AriasAún no hay calificaciones
- Formularios Ejemplo de LlendoDocumento33 páginasFormularios Ejemplo de LlendofarithAún no hay calificaciones
- SOE.568 (08-22) Solicitud Microcrédito, Credisocial Productivo, CrediEmprendeBDV Persona JurídicaDocumento4 páginasSOE.568 (08-22) Solicitud Microcrédito, Credisocial Productivo, CrediEmprendeBDV Persona JurídicaManuel NuñezAún no hay calificaciones
- SOLICITUD INDEMNIZACIÓN DESEMPLEODocumento2 páginasSOLICITUD INDEMNIZACIÓN DESEMPLEOJoyce EscorciaAún no hay calificaciones
- Fondo de Crédito Com. Ind.Documento5 páginasFondo de Crédito Com. Ind.Danny HernàndezAún no hay calificaciones
- Planilla para Personas JuridicasDocumento18 páginasPlanilla para Personas JuridicasMadre Teresa SaludAún no hay calificaciones
- SOE.531 (08-22) Solicitud de Liberación de Hipoteca Por Adquisición de Vivienda PrincipalDocumento1 páginaSOE.531 (08-22) Solicitud de Liberación de Hipoteca Por Adquisición de Vivienda Principalcreaciones Veru100% (2)
- Formularios de LicitacionDocumento52 páginasFormularios de LicitacionAdrian ChambillaAún no hay calificaciones
- Ficha de ClienteDocumento2 páginasFicha de ClienteRicardo Lissabet CalañaAún no hay calificaciones
- Formularios 144Documento12 páginasFormularios 144David PacoAún no hay calificaciones
- Presentación de PropuestaDocumento12 páginasPresentación de PropuestaR Deyvid MachacaAún no hay calificaciones
- FORMULARIOSDocumento9 páginasFORMULARIOSGuzman ArNelAún no hay calificaciones
- Formato de Inscripción de Proveedores Persona JurídicaDocumento2 páginasFormato de Inscripción de Proveedores Persona JurídicaSENA 1067956Aún no hay calificaciones
- Liberacion HipotecasDocumento2 páginasLiberacion HipotecasArturo Navas0% (1)
- 1 PropuestaadministrativaDocumento4 páginas1 PropuestaadministrativaSimon Moises Michel UstarizAún no hay calificaciones
- Ministerio Publico - Santa CruzDocumento9 páginasMinisterio Publico - Santa Cruztop laserAún no hay calificaciones
- Formularios DBSERDocumento30 páginasFormularios DBSERRudyGary100% (1)
- FORMULARIODocumento2 páginasFORMULARIOClara HurtadoAún no hay calificaciones
- SOE531 Liberacion Adquisicion Vivienda PpalDocumento2 páginasSOE531 Liberacion Adquisicion Vivienda PpalAbg Richard Jose Ramirez67% (3)
- Consentimiento 10 902 213 004386Documento168 páginasConsentimiento 10 902 213 004386Mictlán Salgado AlexAún no hay calificaciones
- Lista de Chequeo Contratación Directa - Persona JuridicaDocumento4 páginasLista de Chequeo Contratación Directa - Persona JuridicajltharistizabalAún no hay calificaciones
- Formularios AEVDocumento214 páginasFormularios AEVRodrigo Rios SuarezAún no hay calificaciones
- H01280S (201901) Change Request PDFDocumento2 páginasH01280S (201901) Change Request PDFNicole CastroAún no hay calificaciones
- Forms requisitosNuevosConsultoresDocumento7 páginasForms requisitosNuevosConsultoresMax LopezAún no hay calificaciones
- GR 001 DIGITAL EDITABLE Solicitud Del Seguro Tomador PDFDocumento2 páginasGR 001 DIGITAL EDITABLE Solicitud Del Seguro Tomador PDFYuri Marcela Trujillo M100% (1)
- 0 Formulario Único para EmpresasDocumento3 páginas0 Formulario Único para EmpresasResponsabilidad SocialAún no hay calificaciones
- Solicitud de Seguro Ramo Automóvil V8Documento10 páginasSolicitud de Seguro Ramo Automóvil V8Leny Ávila OrtegaAún no hay calificaciones
- Ficha Del Proceso de ContrataciónDocumento2 páginasFicha Del Proceso de ContrataciónmauforondaAún no hay calificaciones
- 0288 2022 900465319 23 1Documento2 páginas0288 2022 900465319 23 1albaniljessica2019Aún no hay calificaciones
- 912 835 Aseg 097 Desempleo e Incapacidad Total y TemporalDocumento3 páginas912 835 Aseg 097 Desempleo e Incapacidad Total y Temporalfrancisco gayosso vargasAún no hay calificaciones
- Formulario Solicitud de Adhesion EmpresaDocumento2 páginasFormulario Solicitud de Adhesion Empresaxnskiii07Aún no hay calificaciones
- Ficha Del Proceso de Contratación: 11/4/2023 15:00:38 Rsicprocesoficha Página 1 de 2Documento2 páginasFicha Del Proceso de Contratación: 11/4/2023 15:00:38 Rsicprocesoficha Página 1 de 2Erick Bladimir SarabiaAún no hay calificaciones
- Ficha de Cliente - IIDocumento2 páginasFicha de Cliente - IIjulioAún no hay calificaciones
- Formularios de Compra de FiltrosDocumento11 páginasFormularios de Compra de FiltrosHERNANDO CASTILLOAún no hay calificaciones
- 4.formularios DBCDocumento18 páginas4.formularios DBCCarlos ChoqueAún no hay calificaciones
- YURICopia de GC-F307 Certificacion de Supervision de ContratosDocumento2 páginasYURICopia de GC-F307 Certificacion de Supervision de ContratosVIVIANA GODOYAún no hay calificaciones
- Formato de Inscripción de Proveedores Persona Jurídica PDFDocumento2 páginasFormato de Inscripción de Proveedores Persona Jurídica PDFLuis RobayoAún no hay calificaciones
- Organo Judicial OruroDocumento7 páginasOrgano Judicial OruroManuel Oscar RodriguezAún no hay calificaciones
- Formularios 1Documento23 páginasFormularios 1Mario SalazarAún no hay calificaciones
- Solicitud de Credito Carterizado Persona JuridicaDocumento9 páginasSolicitud de Credito Carterizado Persona JuridicaJorber PabonAún no hay calificaciones
- Form 250Documento1 páginaForm 250ALEIDA JEREZ RUIZAún no hay calificaciones
- Ficha Del Proceso de Contratación: 9/1/2024 16:33:15 Rsicprocesoficha Página 1 de 2Documento2 páginasFicha Del Proceso de Contratación: 9/1/2024 16:33:15 Rsicprocesoficha Página 1 de 2Jose Manuel Arias MedinaAún no hay calificaciones
- Colfondos U-6325 Sol - Vinc - o - Tras - PVDocumento8 páginasColfondos U-6325 Sol - Vinc - o - Tras - PVRomuloPerdomoBonnellsAún no hay calificaciones
- Formularios A InteraccionDocumento15 páginasFormularios A InteraccionEinar Fuentes CayojaAún no hay calificaciones
- Plan 21 ContratoDocumento36 páginasPlan 21 ContratoLuis SifontesAún no hay calificaciones
- Formato - Inscripion - Proveedores GEN +Documento2 páginasFormato - Inscripion - Proveedores GEN +JUANPANIAGUAAún no hay calificaciones
- Acta de Liquidacion de Contrato 040-2017 - Fabio German Velasquez SotoDocumento3 páginasActa de Liquidacion de Contrato 040-2017 - Fabio German Velasquez SotoYobanny PadillaAún no hay calificaciones
- ENDE-2016-063Documento13 páginasENDE-2016-063Wilson WilliamAún no hay calificaciones
- LLANTAS para maquinaria pesada y semipesadaDocumento9 páginasLLANTAS para maquinaria pesada y semipesadaLimbert PatonAún no hay calificaciones
- Planilla Crédito Agropecuario-PjDocumento3 páginasPlanilla Crédito Agropecuario-PjleonardollatAún no hay calificaciones
- Formulario Conocimiento de Proveedor PDFDocumento2 páginasFormulario Conocimiento de Proveedor PDFJason MoralesAún no hay calificaciones
- 02 194 - FORMATO PARA INSCRIPCION DE PROVEEDORES - PERSONA NATURAL - CompressedDocumento2 páginas02 194 - FORMATO PARA INSCRIPCION DE PROVEEDORES - PERSONA NATURAL - CompressedMaria Fernanda PiragautaAún no hay calificaciones
- Formulario 200Documento1 páginaFormulario 200Mijail C. Muriel ZambranaAún no hay calificaciones
- Nueva Ficha de Solicitud - ClientesDocumento2 páginasNueva Ficha de Solicitud - ClientesZali Ceyda V. VelasquezAún no hay calificaciones
- Formulario 500 Valle DoradoDocumento1 páginaFormulario 500 Valle DoradoTeddy Márquez DíazAún no hay calificaciones
- Comfenalco ValleDocumento5 páginasComfenalco ValleTaty_9606Aún no hay calificaciones
- Qué Es La Memoria PROMDocumento12 páginasQué Es La Memoria PROMLuis MoralesAún no hay calificaciones
- Lectura 1 - Una Experiencia Con La Competencia Aprendizaje AutonomoDocumento14 páginasLectura 1 - Una Experiencia Con La Competencia Aprendizaje AutonomoAstrid Falla BarbozaAún no hay calificaciones
- Matriz de Bloqueo BOLTER 99-1Documento2 páginasMatriz de Bloqueo BOLTER 99-1Franco100% (1)
- Tipos de MicroscopiosDocumento5 páginasTipos de MicroscopiosNancyAún no hay calificaciones
- Estadísticas de Como Afecta o Beneficia La Inteligencia Artificial en El FuturoDocumento8 páginasEstadísticas de Como Afecta o Beneficia La Inteligencia Artificial en El FuturoGenaro Mendoza MartinezAún no hay calificaciones
- Mecatrónica ProfinetDocumento22 páginasMecatrónica ProfinetGERMANAún no hay calificaciones
- Errores Mas Ffrecuentes en PCDocumento4 páginasErrores Mas Ffrecuentes en PCMasiel Del Prado100% (1)
- S08 PTT FluidosDocumento22 páginasS08 PTT FluidosGIAN MARCO LEZMA MENDOZAAún no hay calificaciones
- Clúster de Alto RendimientoDocumento2 páginasClúster de Alto RendimientoMario MorochoAún no hay calificaciones
- Examen C4Documento8 páginasExamen C4Carlos Yair Palacios PalaciosAún no hay calificaciones
- Tarea 4Documento3 páginasTarea 4Edson Emanuel Garc�a L�pezAún no hay calificaciones
- Material DidacticoDocumento22 páginasMaterial DidacticoBrayan Oncoy MoralesAún no hay calificaciones
- Informe Certificación Orden C Aya07088 Aya07089Documento36 páginasInforme Certificación Orden C Aya07088 Aya07089Carlos Guevara100% (1)
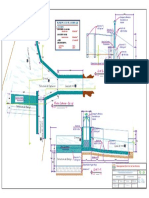
- Captacion BarrajeDocumento1 páginaCaptacion BarrajeE&S IngenieriaServiceAún no hay calificaciones
- Formato de Respuestas - Fase 2 - UnadDocumento7 páginasFormato de Respuestas - Fase 2 - Unadcisco ceroAún no hay calificaciones
- Ediccion de Proyecto ProductivoDocumento27 páginasEdiccion de Proyecto ProductivoDULCE CAJALEON CASOAún no hay calificaciones
- Formato - Peligros - Riesgos - Sec - Economicos SOLUCIONDocumento4 páginasFormato - Peligros - Riesgos - Sec - Economicos SOLUCIONCesar AmadoAún no hay calificaciones
- InecuacionesDocumento24 páginasInecuacionesDaniel VelazquezAún no hay calificaciones
- Programa de AuditoriaDocumento7 páginasPrograma de AuditoriaCarina Castillejo71% (7)
- Teman12nnIntroduccionnAnalisisnEstadistico1 6760c49840530ffDocumento28 páginasTeman12nnIntroduccionnAnalisisnEstadistico1 6760c49840530ffZULMA EDITH AGUDELO MOLINAAún no hay calificaciones
- Mapa Mental - ART. 34 LISR - AVGDocumento2 páginasMapa Mental - ART. 34 LISR - AVGAmisaddai Velázquez GarciaAún no hay calificaciones
- Formato de Trabajo UdabolDocumento12 páginasFormato de Trabajo UdabolDaniela PardoAún no hay calificaciones
- Plan estratégico para incrementar suscriptores de revista de viajes onlineDocumento13 páginasPlan estratégico para incrementar suscriptores de revista de viajes onlineJuan RodriguezAún no hay calificaciones
- Unidad IV: Amplificador OperacionalDocumento35 páginasUnidad IV: Amplificador OperacionalSnowJim16Aún no hay calificaciones
- Auto Bomb AsDocumento39 páginasAuto Bomb Aschamas77Aún no hay calificaciones
- Identificando procesos en Windows con TCPViewDocumento4 páginasIdentificando procesos en Windows con TCPViewJeelon MTAún no hay calificaciones
- FT Nuevo 208 Am22Documento2 páginasFT Nuevo 208 Am22Guillermo VelazquezAún no hay calificaciones
- Las Normas Internacionales de Descripcic3b3n Archivc3adstica1Documento77 páginasLas Normas Internacionales de Descripcic3b3n Archivc3adstica1Pedro Arrieta ChuctayaAún no hay calificaciones
- Una mirada a los procesos unitarios de oxigenación en sistemas RASDocumento7 páginasUna mirada a los procesos unitarios de oxigenación en sistemas RASAngeloAún no hay calificaciones