También podría gustarte
- Sem 03 2017 Ii Dobleces de Alambre AnsasDocumento2 páginasSem 03 2017 Ii Dobleces de Alambre AnsasJHON FRANK ALFREDO JIMENEZ VILLALTA100% (3)
- Tanaka y JhonsonDocumento5 páginasTanaka y JhonsonJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Acv PDFDocumento26 páginasAcv PDFDavid Vargas SerenoAún no hay calificaciones
- Manual de Introducción A Las Ciencias de La SaludDocumento255 páginasManual de Introducción A Las Ciencias de La SaludDenisse Perez100% (4)
- Historia Natural Úlceras Por PresiónDocumento2 páginasHistoria Natural Úlceras Por Presiónmontillo67% (6)
- Oclusión Bilateral BalanceadaDocumento3 páginasOclusión Bilateral BalanceadaJHON FRANK ALFREDO JIMENEZ VILLALTA50% (2)
- Fisiología Del Móvil, Mecanismos y Atención Del Parto PDFDocumento10 páginasFisiología Del Móvil, Mecanismos y Atención Del Parto PDFIgnacioCortésFuentesAún no hay calificaciones
- Cementación Convencional y Adhesiva 1Documento33 páginasCementación Convencional y Adhesiva 1JHON FRANK ALFREDO JIMENEZ VILLALTA100% (1)
- Clase Xii - Prescripción en Infec - OdontoDocumento19 páginasClase Xii - Prescripción en Infec - Odontopiero17cahuaAún no hay calificaciones
- Boletin 027 PDFDocumento6 páginasBoletin 027 PDFPito Perez100% (1)
- Criterios de Rigor CientificoDocumento11 páginasCriterios de Rigor CientificoJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Comunicación Oroantral PDFDocumento9 páginasComunicación Oroantral PDFJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Caries DentalDocumento4 páginasCaries DentalJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Ferulas RigidasDocumento9 páginasFerulas RigidasJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Principios EticosDocumento14 páginasPrincipios EticosJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Características de La Oclusión FuncionalDocumento3 páginasCaracterísticas de La Oclusión FuncionalJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Plano de OclusiónDocumento3 páginasPlano de OclusiónJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Ajuste OclusalDocumento3 páginasAjuste OclusalJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Acto Médico OdontológicoDocumento46 páginasActo Médico OdontológicoJHON FRANK ALFREDO JIMENEZ VILLALTA0% (1)
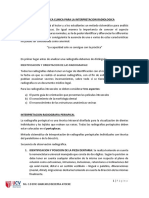
- Imagenologia Guia Clinica EbDocumento20 páginasImagenologia Guia Clinica EbJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Guardias en Exodoncias Que Los Operadores Zurdos Deben Realizar en Cirugía BucalDocumento105 páginasGuardias en Exodoncias Que Los Operadores Zurdos Deben Realizar en Cirugía BucalJHON FRANK ALFREDO JIMENEZ VILLALTAAún no hay calificaciones
- Trabajo de Monografia Previo para Optar Al Titulo De: Licenciado Químico FarmacéuticoDocumento57 páginasTrabajo de Monografia Previo para Optar Al Titulo De: Licenciado Químico FarmacéuticoDavAún no hay calificaciones
- VeraDocumento1 páginaVeraMaria FloresAún no hay calificaciones
- Resultado Del Análisis: Ref:Compaia Minera Antamina S.A. SEXO:Hombre EDAD:26 AñosDocumento2 páginasResultado Del Análisis: Ref:Compaia Minera Antamina S.A. SEXO:Hombre EDAD:26 AñosBryan Guiomar Beteta PantojaAún no hay calificaciones
- Consentimiento Informado FisioterapiaDocumento3 páginasConsentimiento Informado FisioterapiaEduardoAún no hay calificaciones
- Practica 3 AdenovirusDocumento6 páginasPractica 3 AdenovirusJerry Leonardo Rojano SilvaAún no hay calificaciones
- Sindromes VestibularesDocumento12 páginasSindromes VestibularesEvelyn SchellAún no hay calificaciones
- Caso Clinico Obstruccion IntestinalDocumento6 páginasCaso Clinico Obstruccion IntestinalAnderson TipantuñaAún no hay calificaciones
- Autorizaciones Anderson MolinaDocumento2 páginasAutorizaciones Anderson MolinaAnderson Molina BejaranoAún no hay calificaciones
- Historia Natural de La EnfermdadDocumento59 páginasHistoria Natural de La EnfermdadBlanca Mendoza Garcia100% (1)
- Certificados Interjurisdiccional 28-02-2018Documento342 páginasCertificados Interjurisdiccional 28-02-2018padremanuellacunzaAún no hay calificaciones
- Evidencia 1: Informe "Mis Expectativas en La Organización Receptora Como Estudiante de Servicio Social"Documento7 páginasEvidencia 1: Informe "Mis Expectativas en La Organización Receptora Como Estudiante de Servicio Social"Nelda Fernanda AlejandroAún no hay calificaciones
- Cómo Influye La Depresión en La Diabetes en El Adulto MayorDocumento39 páginasCómo Influye La Depresión en La Diabetes en El Adulto MayorAmazonica leeAún no hay calificaciones
- Fibrodisplasia Osificante ProgresivaDocumento6 páginasFibrodisplasia Osificante ProgresivaDiego SamaelAún no hay calificaciones
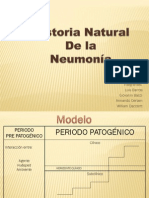
- HN NeumoniaDocumento16 páginasHN NeumoniaBilly Daccarett BojaniniAún no hay calificaciones
- Bitacora de Practica Primeros AuxiliosDocumento7 páginasBitacora de Practica Primeros AuxiliosJaiber AvilaAún no hay calificaciones
- Vih - Sida: Dr. Miguel Martin Romero Dominguez InfectologiaDocumento45 páginasVih - Sida: Dr. Miguel Martin Romero Dominguez InfectologiaAlejandra Castañon CoronaAún no hay calificaciones
- Ganglios LinfáticosDocumento2 páginasGanglios LinfáticosCarlos RuizAún no hay calificaciones
- Bitacora #6Documento3 páginasBitacora #6David AlmaralesAún no hay calificaciones
- Resolución Caso EdemaDocumento3 páginasResolución Caso EdemaLinterna VerdeAún no hay calificaciones
- Fitoterapia Integrativa 2023Documento6 páginasFitoterapia Integrativa 2023mingo.boxing.clAún no hay calificaciones
- Reto 6 ValeriaDocumento3 páginasReto 6 Valeriavaleria martinezAún no hay calificaciones
- Caso Clinico ApendisectomiaDocumento25 páginasCaso Clinico ApendisectomiaAdrián BaqueAún no hay calificaciones
- Biondi, Radiologia (ES PRIMERA EDICION)Documento28 páginasBiondi, Radiologia (ES PRIMERA EDICION)Federico 199Aún no hay calificaciones
- Hipertension ArterialDocumento9 páginasHipertension ArterialRosa FloresAún no hay calificaciones