También podría gustarte
- Normas de VancouverDocumento50 páginasNormas de VancouverwiritaAún no hay calificaciones
- Formulación del problema de investigaciónDocumento24 páginasFormulación del problema de investigaciónwiritaAún no hay calificaciones
- Alvlitis 1Documento5 páginasAlvlitis 1Lex Puma IdmeAún no hay calificaciones
- Iii. Marco TeoricoDocumento22 páginasIii. Marco TeoricowiritaAún no hay calificaciones
- AlveolitisDocumento5 páginasAlveolitiselianaAún no hay calificaciones
- Evaluacion Clinica en La Cicatrizacion Del AlveoloDocumento6 páginasEvaluacion Clinica en La Cicatrizacion Del AlveolowiritaAún no hay calificaciones
- Hidroxido de Calcio Paradigma ClinicoDocumento32 páginasHidroxido de Calcio Paradigma Clinicowirita0% (1)
- Cosme Gay 1 PDFDocumento44 páginasCosme Gay 1 PDFJccmAún no hay calificaciones
- Manual Del Cuidado Del Perro IIDocumento16 páginasManual Del Cuidado Del Perro IInoslen borjasAún no hay calificaciones
- Ecorregiones Región SierraDocumento6 páginasEcorregiones Región SierrawiritaAún no hay calificaciones
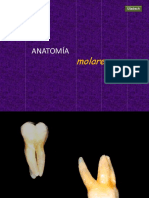
- Anatomía Molares1Documento68 páginasAnatomía Molares1wiritaAún no hay calificaciones
- Ambiente Organizacional ClaseDocumento42 páginasAmbiente Organizacional ClasewiritaAún no hay calificaciones
- Manual endodoncia UFRODocumento132 páginasManual endodoncia UFROBioquimica UplaAún no hay calificaciones
- Cosme Gay 1 PDFDocumento44 páginasCosme Gay 1 PDFJccmAún no hay calificaciones
- AnemiaDocumento3 páginasAnemiawiritaAún no hay calificaciones
- 10-Hiperplasias de La Mucosa BucalDocumento11 páginas10-Hiperplasias de La Mucosa BucalinesgualanAún no hay calificaciones
- Ciclo Menstrual en La MujerDocumento7 páginasCiclo Menstrual en La MujerwiritaAún no hay calificaciones
- Hepatitisb 100301182145 Phpapp02Documento36 páginasHepatitisb 100301182145 Phpapp02wiritaAún no hay calificaciones
- Expo - ShockDocumento88 páginasExpo - ShockwiritaAún no hay calificaciones
- PDF OclusionDocumento20 páginasPDF OclusionwiritaAún no hay calificaciones
- A Conectivo Adiposo PDFDocumento7 páginasA Conectivo Adiposo PDFLuisa MatzkAún no hay calificaciones
- Los Nucleótidos y Los Ácidos NucléicosDocumento7 páginasLos Nucleótidos y Los Ácidos NucléicoswiritaAún no hay calificaciones
- Biomecanica DentalDocumento38 páginasBiomecanica Dentalwirita100% (3)
- Nota de Evolucion PFDocumento4 páginasNota de Evolucion PFJorge Benítez Ramírez100% (1)
- Guías de Procedimientos en ReumatologíaDocumento188 páginasGuías de Procedimientos en ReumatologíaEri HSAún no hay calificaciones
- TRIPTICODocumento2 páginasTRIPTICOAracelly RomeroAún no hay calificaciones
- Taller No. 4 DE PLAN LECTOR 7° Todo Bien Todo BienDocumento1 páginaTaller No. 4 DE PLAN LECTOR 7° Todo Bien Todo BienOscar Alfonso Diaz CruzAún no hay calificaciones
- Qué Es Obstetricia y NeonatologíaDocumento3 páginasQué Es Obstetricia y NeonatologíaVioleta VeraAún no hay calificaciones
- Evaluación de la práctica odontológica integral IIDocumento3 páginasEvaluación de la práctica odontológica integral IIAlex Drago BermudezAún no hay calificaciones
- La Proteína S100 Como Marcador Tumoral en Pacientes Con Melanoma. Estudio Comparativo Con Ganglio Centinela y La Exploración FDG-PETDocumento10 páginasLa Proteína S100 Como Marcador Tumoral en Pacientes Con Melanoma. Estudio Comparativo Con Ganglio Centinela y La Exploración FDG-PETMario CastroAún no hay calificaciones
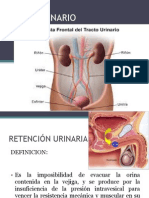
- Sistema UrinarioDocumento74 páginasSistema UrinarioDietry Johanna Lillo UribeAún no hay calificaciones
- V 53 N 2 A 03Documento31 páginasV 53 N 2 A 03Carmen Mejia de CéspedesAún no hay calificaciones
- SOPORTE VITAL SEM y AHA MarybethDocumento1 páginaSOPORTE VITAL SEM y AHA MarybethMarybeth Zurita TorricoAún no hay calificaciones
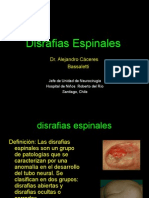
- Disrafias Espinales: Diagnóstico y TratamientoDocumento35 páginasDisrafias Espinales: Diagnóstico y TratamientoShayo LizzyAún no hay calificaciones
- Campaña Mi Primer Laimento Triptico..CorregidoDocumento2 páginasCampaña Mi Primer Laimento Triptico..CorregidoRox SofAún no hay calificaciones
- Cuestionario #3Documento3 páginasCuestionario #3MicheleAlvesBarrosAún no hay calificaciones
- Informe psicológico depresiónDocumento4 páginasInforme psicológico depresiónTulia johana Carreño mendozaAún no hay calificaciones
- Plan médico familiar Monterrey bajo costoDocumento17 páginasPlan médico familiar Monterrey bajo costoEmanuel rodriguezAún no hay calificaciones
- Resiliencia y locus de control en estudiantes de Psicología y Tecnología MédicaDocumento65 páginasResiliencia y locus de control en estudiantes de Psicología y Tecnología Médicamilagros100% (1)
- Plantilla Urgencias Pediacc81tricas Raul WordDocumento12 páginasPlantilla Urgencias Pediacc81tricas Raul WordTrader SpiderAún no hay calificaciones
- Exten. Nuevas Del Huem 2018Documento17 páginasExten. Nuevas Del Huem 2018claudia mendozaAún no hay calificaciones
- Epidemiología veterinaria: métodos y aplicacionesDocumento10 páginasEpidemiología veterinaria: métodos y aplicacionesJuaquin VeterinarioAún no hay calificaciones
- TdahDocumento291 páginasTdahJose A HidalgoAún no hay calificaciones
- triage-clasificacion-victimasDocumento24 páginastriage-clasificacion-victimasABIGAIL ROMAN RAMIREZAún no hay calificaciones
- Xporma 114165 PHPPPDocumento26 páginasXporma 114165 PHPPPlewisantonyAún no hay calificaciones
- 1º ROTAFOLIO HipertencionDocumento6 páginas1º ROTAFOLIO Hipertencionpaola sofia cordova huamaniAún no hay calificaciones
- Quiste GanglionarDocumento10 páginasQuiste GanglionarAlejandro Morales100% (1)
- Miper Cielo AmericanoDocumento15 páginasMiper Cielo AmericanolidiaingeborAún no hay calificaciones
- GPC - Odontologia Mujer GestanteDocumento162 páginasGPC - Odontologia Mujer GestanteAndresFelipeAbrilCamposAún no hay calificaciones
- Poes Lavado de ManoDocumento7 páginasPoes Lavado de ManoNelson NietoAún no hay calificaciones
- Sindrome de DiogenesDocumento5 páginasSindrome de DiogenesIvan BaigorriaAún no hay calificaciones
- Diapositivas )Documento26 páginasDiapositivas )SxNti BustamanteAún no hay calificaciones
- Evaluación PlacentariaDocumento23 páginasEvaluación PlacentariaKarlin ReyesAún no hay calificaciones
- El Monje Que Vendio Su Ferrari: Una Fábula EspiritualDe EverandEl Monje Que Vendio Su Ferrari: Una Fábula EspiritualCalificación: 4.5 de 5 estrellas4.5/5 (1696)
- Resetea tu mente. Descubre de lo que eres capazDe EverandResetea tu mente. Descubre de lo que eres capazCalificación: 5 de 5 estrellas5/5 (196)
- Viaje a través del libro de ejercicios de un curso de milagros. Volumen 1De EverandViaje a través del libro de ejercicios de un curso de milagros. Volumen 1Calificación: 4 de 5 estrellas4/5 (8)
- Los 12 chakras: Desbloquea tus dones espiritualesDe EverandLos 12 chakras: Desbloquea tus dones espiritualesCalificación: 4 de 5 estrellas4/5 (14)
- Las seis etapas definitivas para superar tu divorcioDe EverandLas seis etapas definitivas para superar tu divorcioCalificación: 4.5 de 5 estrellas4.5/5 (10)
- TDAH en Adultos. Cómo Reconocer y Tratar a un Adulto con TDAH en 30 Fáciles PasosDe EverandTDAH en Adultos. Cómo Reconocer y Tratar a un Adulto con TDAH en 30 Fáciles PasosCalificación: 4 de 5 estrellas4/5 (8)
- Solo quiero que sepas: Lo que hemos aprendido y descubierto acerca de las relaciones amorosasDe EverandSolo quiero que sepas: Lo que hemos aprendido y descubierto acerca de las relaciones amorosasCalificación: 5 de 5 estrellas5/5 (38)
- ¡Tómate un respiro! Mindfulness: El arte de mantener la calma en medio de la tempestadDe Everand¡Tómate un respiro! Mindfulness: El arte de mantener la calma en medio de la tempestadCalificación: 5 de 5 estrellas5/5 (198)
- Entrenamiento Científico con pesas: Fitness InteligenteDe EverandEntrenamiento Científico con pesas: Fitness InteligenteCalificación: 5 de 5 estrellas5/5 (3)
- La Tabla Esmeralda: Incluye varias versiones y explicacionesDe EverandLa Tabla Esmeralda: Incluye varias versiones y explicacionesCalificación: 4.5 de 5 estrellas4.5/5 (7)
- Disciplina con amor para adolescentes (Discipline With Love for Adolescents): Guía para llevarte bien con tu adolescente (A Guide for Getting Along Well With Your Adolescent)De EverandDisciplina con amor para adolescentes (Discipline With Love for Adolescents): Guía para llevarte bien con tu adolescente (A Guide for Getting Along Well With Your Adolescent)Calificación: 5 de 5 estrellas5/5 (10)
- Cómo Conversar Con Cualquier Persona: Mejora tus habilidades sociales, desarrolla tu carisma, domina las conversaciones triviales y conviértete en una persona sociable para hacer verdaderos amigos y construir relaciones significativas.De EverandCómo Conversar Con Cualquier Persona: Mejora tus habilidades sociales, desarrolla tu carisma, domina las conversaciones triviales y conviértete en una persona sociable para hacer verdaderos amigos y construir relaciones significativas.Calificación: 5 de 5 estrellas5/5 (54)
- ¡Basta ya de ser un Tipo Lindo! (No More Mr. Nice Guy): Un Plan Probado para Que Obtengas Lo Que Quieras en La Vida El Sexo y El Amor (A Proven Plan for Getting What You Want in Love, Sex and Life)De Everand¡Basta ya de ser un Tipo Lindo! (No More Mr. Nice Guy): Un Plan Probado para Que Obtengas Lo Que Quieras en La Vida El Sexo y El Amor (A Proven Plan for Getting What You Want in Love, Sex and Life)Calificación: 5 de 5 estrellas5/5 (47)
- El oráculo de las diosas: El despertar de lo femenino. Guía de autoconocimientoDe EverandEl oráculo de las diosas: El despertar de lo femenino. Guía de autoconocimientoCalificación: 5 de 5 estrellas5/5 (1)
- La Guía del Estoicismo para Tiempos Modernos: Cómo entender y practicar el estoicismo para una vida plena y tranquila en tiempos modernosDe EverandLa Guía del Estoicismo para Tiempos Modernos: Cómo entender y practicar el estoicismo para una vida plena y tranquila en tiempos modernosCalificación: 5 de 5 estrellas5/5 (23)
- Guía de Telepatía en Español: Cómo Desarrollar tus Habilidades Psíquicas y Desarrollar una Consciencia Extra SensorialDe EverandGuía de Telepatía en Español: Cómo Desarrollar tus Habilidades Psíquicas y Desarrollar una Consciencia Extra SensorialCalificación: 5 de 5 estrellas5/5 (10)
- Mindfulness para principiantes: Medita sin meditarDe EverandMindfulness para principiantes: Medita sin meditarCalificación: 5 de 5 estrellas5/5 (53)
- La conquista del temploDe EverandLa conquista del temploCalificación: 4.5 de 5 estrellas4.5/5 (27)