También podría gustarte
- Respuestas Examen Final PresupuestosDocumento12 páginasRespuestas Examen Final PresupuestosAugusto Alejandro L. Garcia71% (7)
- Propiedades Geométricas de Las Secciones de Los Perfiles ComercialesDocumento9 páginasPropiedades Geométricas de Las Secciones de Los Perfiles Comercialesdenilson jimenez0% (1)
- SIG-M-01 MATRIZ RIESGOS MYC ASOCIADOSDocumento19 páginasSIG-M-01 MATRIZ RIESGOS MYC ASOCIADOSFelipe MendietaAún no hay calificaciones
- Malla Capacitaciones ARL SURA 2024Documento138 páginasMalla Capacitaciones ARL SURA 2024Felipe MendietaAún no hay calificaciones
- Dias Sin AccidentesDocumento1 páginaDias Sin AccidentesFelipe MendietaAún no hay calificaciones
- Encuesta OsteomuscularDocumento4 páginasEncuesta OsteomuscularFelipe MendietaAún no hay calificaciones
- Objetivos de Seguridad y Salud en El TrabajoDocumento1 páginaObjetivos de Seguridad y Salud en El TrabajoFelipe MendietaAún no hay calificaciones
- FT-SST - Hoja de Vida ArnesDocumento3 páginasFT-SST - Hoja de Vida ArnesFelipe MendietaAún no hay calificaciones
- Fto-Sst-26 Formato Evaluacion Capacitaciones SstaDocumento2 páginasFto-Sst-26 Formato Evaluacion Capacitaciones SstaFelipe MendietaAún no hay calificaciones
- Mecanismo Rendicion de CuentasDocumento4 páginasMecanismo Rendicion de CuentasFelipe MendietaAún no hay calificaciones
- Funciones de TrabajadoresDocumento2 páginasFunciones de TrabajadoresFelipe MendietaAún no hay calificaciones
- Instructivo Fumigadora de EspaldaDocumento1 páginaInstructivo Fumigadora de EspaldaFelipe MendietaAún no hay calificaciones
- Permiso de Trabajo 2022Documento4 páginasPermiso de Trabajo 2022Felipe MendietaAún no hay calificaciones
- Procedimiento Armado y Vaciado de Escalas en ConcretoDocumento5 páginasProcedimiento Armado y Vaciado de Escalas en ConcretoFelipe Mendieta100% (1)
- 03 Form-RuidoDocumento8 páginas03 Form-RuidoFelipe MendietaAún no hay calificaciones
- Pve-Sst-02 Programa de Vigilancia Epidemiologica Frente Al Riesgo Psicosocial (Salud Mental)Documento2 páginasPve-Sst-02 Programa de Vigilancia Epidemiologica Frente Al Riesgo Psicosocial (Salud Mental)Felipe MendietaAún no hay calificaciones
- STD Máquina Tronzadora MetalDocumento1 páginaSTD Máquina Tronzadora MetalFelipe MendietaAún no hay calificaciones
- 01 Pve-RuidoDocumento32 páginas01 Pve-RuidoFelipe MendietaAún no hay calificaciones
- Capacitacion Prevencion de Consumo Alcohol Drogas y Sustancia PsicoaptivasDocumento15 páginasCapacitacion Prevencion de Consumo Alcohol Drogas y Sustancia PsicoaptivasFelipe MendietaAún no hay calificaciones
- Folleto Prevencion de Consumo de Alcohol Drogas y TabaquismoDocumento2 páginasFolleto Prevencion de Consumo de Alcohol Drogas y TabaquismoFelipe Mendieta100% (2)
- Guia de Salud Mental y Lineas de Atencion para Este Riesgo PsicosocialDocumento6 páginasGuia de Salud Mental y Lineas de Atencion para Este Riesgo PsicosocialFelipe MendietaAún no hay calificaciones
- STD Trabajos en AlturasDocumento1 páginaSTD Trabajos en AlturasFelipe MendietaAún no hay calificaciones
- Practico2 Mec 260 2-2019Documento2 páginasPractico2 Mec 260 2-2019Luis Miguel SequeliAún no hay calificaciones
- Caso Estado de CostosDocumento1 páginaCaso Estado de CostosKrlos CristobalAún no hay calificaciones
- Copia de Traige PaDocumento49 páginasCopia de Traige PaNohemi CastruitaAún no hay calificaciones
- Taller Pronósticos de La DemandaDocumento2 páginasTaller Pronósticos de La DemandaJairo SierraAún no hay calificaciones
- PCH CarDocumento1 páginaPCH CarjorgeAún no hay calificaciones
- Documentacion de CompiladorDocumento8 páginasDocumentacion de CompiladorDavid HurtadoAún no hay calificaciones
- Cotización N°01 - Ie N°00616Documento7 páginasCotización N°01 - Ie N°00616Julver nilo Tinoco guevaraAún no hay calificaciones
- Tofa Proyecto TesisDocumento2 páginasTofa Proyecto TesisAmerica SerranoAún no hay calificaciones
- Tablas de Conversión de Fechas IslámicasDocumento212 páginasTablas de Conversión de Fechas IslámicasFernandoMoraAún no hay calificaciones
- De Medios Alternativos A Medios CiudadanosDocumento13 páginasDe Medios Alternativos A Medios CiudadanosEugenia ScoppettaAún no hay calificaciones
- Analisis Dimensional IIDocumento5 páginasAnalisis Dimensional IIWilberth LevitaAún no hay calificaciones
- Masa CríticaDocumento2 páginasMasa CríticaRodrigo OliveraAún no hay calificaciones
- Guía Del Constructor EcuadorDocumento80 páginasGuía Del Constructor EcuadorJavier Guaicha Castillo100% (1)
- Anticonceptivos InyectablesDocumento25 páginasAnticonceptivos InyectablesNicolas Patricio Sitja100% (1)
- Pauta Mantencion Excavadora CAT 320..Documento6 páginasPauta Mantencion Excavadora CAT 320..KatherinE Rodriguez100% (2)
- Guia Generica para La Presentacion Del Perfil de TFG UtepsaDocumento7 páginasGuia Generica para La Presentacion Del Perfil de TFG UtepsaRonald Miranda Durán0% (1)
- Peces InformeDocumento10 páginasPeces InformeKevin DiazAún no hay calificaciones
- Macroeconomia Iii 2 Bim Tablet 1101467Documento9 páginasMacroeconomia Iii 2 Bim Tablet 1101467Juan RealAún no hay calificaciones
- Valores FormDocumento4 páginasValores Formadriana portelaAún no hay calificaciones
- 5 - Nonio Recto (Lectura)Documento6 páginas5 - Nonio Recto (Lectura)Carlos Cervantes DiazAún no hay calificaciones
- Manual Sanacion Cuantica 18 Abr 2017 V2Documento23 páginasManual Sanacion Cuantica 18 Abr 2017 V2Loreto YpazAún no hay calificaciones
- Vectores P.P. UNPRGDocumento4 páginasVectores P.P. UNPRGLeonardo WalterAún no hay calificaciones
- La Cadena Del Valor de PorterDocumento17 páginasLa Cadena Del Valor de PorterManuel AlejandroAún no hay calificaciones
- Informe Construcción. Impresoras 3DDocumento9 páginasInforme Construcción. Impresoras 3DMalakai AstoAún no hay calificaciones
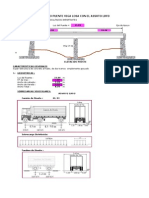
- Hoja de Calculo Puente Viga Losa-Diseño de Viga (Configurado 14 Mayo 2011)Documento138 páginasHoja de Calculo Puente Viga Losa-Diseño de Viga (Configurado 14 Mayo 2011)extable100% (7)
- Listado de Libros Ies San Isidro 2022-2023Documento5 páginasListado de Libros Ies San Isidro 2022-2023Martha EscarpaAún no hay calificaciones
- Fabricacion Artesanal de CuchillosDocumento2 páginasFabricacion Artesanal de CuchillosSeba CabezaRapadaAún no hay calificaciones
- 1829 Farmacopea UniversalDocumento538 páginas1829 Farmacopea UniversalGamy HernandezAún no hay calificaciones