También podría gustarte
- 19.farmacos AnticoagulantesDocumento3 páginas19.farmacos AnticoagulantesMarlen Becerra100% (6)
- Constancia AntecedentesDocumento1 páginaConstancia AntecedentesRicardo BeltranAún no hay calificaciones
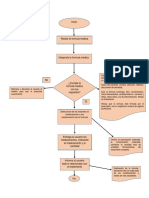
- Flujograma de DispensacionDocumento1 páginaFlujograma de Dispensacionvcv lovato74% (19)
- Carta de Terminos y Condiciones NPIE2Documento2 páginasCarta de Terminos y Condiciones NPIE2adrianAún no hay calificaciones
- Acta de nacimiento de Grace Terrazas RicoDocumento1 páginaActa de nacimiento de Grace Terrazas RicoPriscila TerrazasAún no hay calificaciones
- Acta Nacimiento PDFDocumento1 páginaActa Nacimiento PDFJacobo EsparzaAún no hay calificaciones
- Forma Migratoria 00010597166FEDocumento2 páginasForma Migratoria 00010597166FEDaniel Efros RuizAún no hay calificaciones
- Cita de InfonavitDocumento1 páginaCita de Infonavitbereshan lopezAún no hay calificaciones
- Fármacos AntidiabéticosDocumento31 páginasFármacos AntidiabéticosGracil Antonio Wicab CheAún no hay calificaciones
- Acuse de Cedula Unica - CSI-EBS-2122-000308251Documento2 páginasAcuse de Cedula Unica - CSI-EBS-2122-000308251Marvin ValdezAún no hay calificaciones
- Kardex de Medicamentos C.S Arcapamba 2020Documento201 páginasKardex de Medicamentos C.S Arcapamba 2020Wilson LoaizaAún no hay calificaciones
- Recibo 530110302133 AgostoDocumento2 páginasRecibo 530110302133 AgostoDenis ArguellesAún no hay calificaciones
- EncuadernacionDocumento1 páginaEncuadernaciongraficos la fuenteAún no hay calificaciones
- Formato - Universal - SEDENA CARTILLADocumento4 páginasFormato - Universal - SEDENA CARTILLAC.P. GUSTAVO DominguezAún no hay calificaciones
- Verifica tu CURP enDocumento1 páginaVerifica tu CURP enRigoberto Ignacio JesusAún no hay calificaciones
- PACJ670810HDFLRN09Documento1 páginaPACJ670810HDFLRN09Arturo PlascenciaAún no hay calificaciones
- CartaAntecedentesPenalesDocumento1 páginaCartaAntecedentesPenalesrigoberto MartinezAún no hay calificaciones
- Acta de Nacimiento en BlancoDocumento1 páginaActa de Nacimiento en BlancoLuis RosalesAún no hay calificaciones
- Certificado de VacunaciónDocumento1 páginaCertificado de VacunaciónLuis RosasAún no hay calificaciones
- Certificado de ComuniónDocumento2 páginasCertificado de ComuniónMailen ValerianoAún no hay calificaciones
- Permiso MigracionDocumento3 páginasPermiso MigracionRoy Navarrete100% (1)
- Un Rif VenezolanoDocumento1 páginaUn Rif Venezolanoalex mataAún no hay calificaciones
- Constancia no antecedentes penalesDocumento1 páginaConstancia no antecedentes penalesAriel HernandezAún no hay calificaciones
- COVID-19 Vaccination Record Card CDC (8!17!2020)Documento2 páginasCOVID-19 Vaccination Record Card CDC (8!17!2020)pifyuyastaAún no hay calificaciones
- Licencia de Conducir: Licencia Del Ciudadano (A)Documento1 páginaLicencia de Conducir: Licencia Del Ciudadano (A)Yohandri Artigas100% (1)
- Registro de vacunación COVID-19Documento2 páginasRegistro de vacunación COVID-19SlychenkoAún no hay calificaciones
- Poliza MapfreDocumento5 páginasPoliza MapfreMiguel MorenoAún no hay calificaciones
- Acta de Nacimiento AATM800130MVZBBR08Documento1 páginaActa de Nacimiento AATM800130MVZBBR08Victor Manuel Jr.Aún no hay calificaciones
- Acta NacimientoDocumento1 páginaActa Nacimientoabizstuan.140999Aún no hay calificaciones
- CV Mauro Gzlz 6to Sem ContaduríaDocumento7 páginasCV Mauro Gzlz 6to Sem Contaduríagraficos la fuente0% (2)
- Acta de Nacimiento LOAJ850902HMNPRL05Documento1 páginaActa de Nacimiento LOAJ850902HMNPRL05julianAún no hay calificaciones
- Certificado Vacunacion CovidDocumento1 páginaCertificado Vacunacion Covidtramitessemideg comercializadoraAún no hay calificaciones
- Certificado Mi VacunaDocumento1 páginaCertificado Mi VacunaDaniela DøHeAún no hay calificaciones
- Certificado de VacunacionDocumento1 páginaCertificado de VacunacionJudith CastellanosAún no hay calificaciones
- Licencia de Conducir PDFDocumento1 páginaLicencia de Conducir PDFJean KainAún no hay calificaciones
- Formato UniversalDocumento7 páginasFormato UniversalRicardo Sanchez Sanchez100% (1)
- Dni New YorkDocumento2 páginasDni New YorkDiego Paredes CastilloAún no hay calificaciones
- Constancia de Situación Fiscal Enero 2024Documento3 páginasConstancia de Situación Fiscal Enero 2024ernesto chavez ruizAún no hay calificaciones
- Instructivo ESPE Firma Electrònica - RESOLUCION-2020-060Documento16 páginasInstructivo ESPE Firma Electrònica - RESOLUCION-2020-060Arianna DrouetAún no hay calificaciones
- Aewebpoldiae34761124 PDFDocumento11 páginasAewebpoldiae34761124 PDFsergioAún no hay calificaciones
- Acta de NacimientoDocumento2 páginasActa de NacimientoDaniel MedAún no hay calificaciones
- Certificado de nacimiento de Amilkar Zoe Balderas SánchezDocumento1 páginaCertificado de nacimiento de Amilkar Zoe Balderas SánchezZoe BalderasAún no hay calificaciones
- GEJ-CTN-R-23 Autorización Tratamiento Datos Partes Interesadas V2Documento2 páginasGEJ-CTN-R-23 Autorización Tratamiento Datos Partes Interesadas V2alfonso jimenezAún no hay calificaciones
- Solicitud de Registro en Administradora de Fondos para El RetiroDocumento14 páginasSolicitud de Registro en Administradora de Fondos para El RetiroSelene RodriguezAún no hay calificaciones
- Cartilla Militar Nacional Requisitos TrámiteDocumento1 páginaCartilla Militar Nacional Requisitos TrámiteNegryta MayaAún no hay calificaciones
- FormularioDocumento4 páginasFormularioMaria Elina Paredes Figueroa100% (1)
- Recomendaciones para Tarjeta de Movilidad FronterizaDocumento2 páginasRecomendaciones para Tarjeta de Movilidad Fronterizaorlando hidalgoAún no hay calificaciones
- InsaludDocumento2 páginasInsaludGregory MontesinoAún no hay calificaciones
- Certificado Vacunación COVID-19Documento2 páginasCertificado Vacunación COVID-19leon andradeAún no hay calificaciones
- 0 PDFDocumento1 página0 PDFJoel YáñezAún no hay calificaciones
- BoletoElectronico PDFDocumento1 páginaBoletoElectronico PDFJoel AlexisAún no hay calificaciones
- Fcibe531315Documento2 páginasFcibe531315dani righaAún no hay calificaciones
- Obtén tu Certificado de Antecedentes PenalesDocumento1 páginaObtén tu Certificado de Antecedentes PenalesJohan ManuelAún no hay calificaciones
- SuraDocumento3 páginasSuraHumBert Rd GonzalezAún no hay calificaciones
- AMSRT 110210 EditableDocumento9 páginasAMSRT 110210 EditableJorge Armando Barrera CoyocAún no hay calificaciones
- RecetaDocumento4 páginasRecetaGamaliel GamaAún no hay calificaciones
- ControlSanitarioVueloQRDocumento1 páginaControlSanitarioVueloQRLuis Solana Ureña0% (2)
- Certificado de No Antecedentes PenalesDocumento1 páginaCertificado de No Antecedentes PenalesIsabel Hernandez100% (1)
- PDF Estado de Cuenta EditableDocumento5 páginasPDF Estado de Cuenta EditableLuis OcampoAún no hay calificaciones
- Certificado vacunación COVIDDocumento1 páginaCertificado vacunación COVIDEduardo Andrade0% (1)
- Certificado Vacunacion ARMANDO ENRIQUEZDocumento1 páginaCertificado Vacunacion ARMANDO ENRIQUEZJOSE LUISAún no hay calificaciones
- Tiie 8829 PDFDocumento1 páginaTiie 8829 PDFOscar MartinezAún no hay calificaciones
- Nuevo formato Licencia Conducir INTTDocumento1 páginaNuevo formato Licencia Conducir INTTWilfredo El MagoAún no hay calificaciones
- Vaccine 1Documento2 páginasVaccine 1Avya BrutusAún no hay calificaciones
- Vacuna UsaDocumento2 páginasVacuna UsaEbenezer Hernández VargasAún no hay calificaciones
- Shot Card SpanishDocumento2 páginasShot Card SpanishBruse WayneAún no hay calificaciones
- Port AdaDocumento2 páginasPort Adagraficos la fuenteAún no hay calificaciones
- Port AdaDocumento2 páginasPort Adagraficos la fuenteAún no hay calificaciones
- IPUC presenta su Pensum Nacional de Escuela Dominical: Integral, Inspirado y EconómicoDocumento2 páginasIPUC presenta su Pensum Nacional de Escuela Dominical: Integral, Inspirado y Económicograficos la fuenteAún no hay calificaciones
- AlaskaDocumento1 páginaAlaskagraficos la fuenteAún no hay calificaciones
- Supertienda CafanDocumento1 páginaSupertienda Cafangraficos la fuenteAún no hay calificaciones
- AntorchaDocumento1 páginaAntorchagraficos la fuenteAún no hay calificaciones
- Cartilla FinalDocumento11 páginasCartilla Finalgraficos la fuenteAún no hay calificaciones
- Ensayo Sobre La DrogadiccionDocumento7 páginasEnsayo Sobre La DrogadiccionJuan Jimenez JiménezAún no hay calificaciones
- Receta MedicaDocumento2 páginasReceta MedicaELVIA BENANCIOAún no hay calificaciones
- Listado General Agosto 2020Documento16 páginasListado General Agosto 2020Julian SanchezAún no hay calificaciones
- FarmacologíaDocumento38 páginasFarmacologíaDomenica PeñaAún no hay calificaciones
- Brote Epidémico de Intoxicación Alimentaria Por Cannabinoides - Marlon VergaraDocumento3 páginasBrote Epidémico de Intoxicación Alimentaria Por Cannabinoides - Marlon VergaraMarlon Vergara MonterrozaAún no hay calificaciones
- RECETA Ever CorregidaDocumento1 páginaRECETA Ever Corregidadante nefilimAún no hay calificaciones
- ATB Más Usados en OdontologiaDocumento3 páginasATB Más Usados en OdontologiaPía Carolina RomoAún no hay calificaciones
- Sem 3 FarmaDocumento4 páginasSem 3 Farmajuan saezAún no hay calificaciones
- Cálculos para administración intravenosaDocumento9 páginasCálculos para administración intravenosaLuz CetAún no hay calificaciones
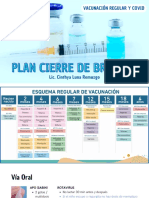
- Plan Cierre de Brechas Vacunación Regular y CovidDocumento24 páginasPlan Cierre de Brechas Vacunación Regular y CovidGestión y Desarrollo InmobiliarioAún no hay calificaciones
- VADEMECUM GES PATDocumento15 páginasVADEMECUM GES PATJessicaAlejandraCastilloLopezAún no hay calificaciones
- Requisitos para Presentar La Informacion SEPB 13112018Documento16 páginasRequisitos para Presentar La Informacion SEPB 13112018Idalia OrtegaAún no hay calificaciones
- Conceptos Fundamentales en DrogodependenciasDocumento55 páginasConceptos Fundamentales en DrogodependenciasMisty MirandaAún no hay calificaciones
- Modelo de Indicación para InternaciónDocumento5 páginasModelo de Indicación para Internaciónisabelle soaresAún no hay calificaciones
- Metformina Upana Primer Año GloriaDocumento33 páginasMetformina Upana Primer Año GloriaDj-Josman ManoloAún no hay calificaciones
- Antibioticos CIRUGIA IDocumento12 páginasAntibioticos CIRUGIA IRobinson Vasquez ChavezAún no hay calificaciones
- Anestesia Cuadro Comparativo (3489)Documento7 páginasAnestesia Cuadro Comparativo (3489)JavierAlvarezAún no hay calificaciones
- ToxisíndromesDocumento28 páginasToxisíndromeschristianklaus94Aún no hay calificaciones
- Perebron Infantil 28mg - 5mlDocumento2 páginasPerebron Infantil 28mg - 5mlAndrea CamiciaAún no hay calificaciones
- Terapia SMARTDocumento16 páginasTerapia SMARTquimegiAún no hay calificaciones
- Cuadros Bacterias Gram Positivas y Gram Negativas Pamela CruzDocumento7 páginasCuadros Bacterias Gram Positivas y Gram Negativas Pamela CruzGabriel Antonio Cedeño SánchezAún no hay calificaciones
- Lista Básica de Medicamentos ReguladosDocumento69 páginasLista Básica de Medicamentos ReguladosNeil J. Rincón M.100% (1)
- Practica de FarmacoDocumento14 páginasPractica de FarmacoGino TámaraAún no hay calificaciones
- Ventajas de Decadurabolin OficialDocumento2 páginasVentajas de Decadurabolin Oficialwealthyelite576Aún no hay calificaciones
- IntoxicacionesDocumento6 páginasIntoxicacionesRissi RodriguezAún no hay calificaciones
- Examen Auxiliar PPT 2. 2014Documento8 páginasExamen Auxiliar PPT 2. 2014peramotaAún no hay calificaciones