También podría gustarte
- Tabla de EstiramientosDocumento4 páginasTabla de EstiramientosVíctor Muñoz LópezAún no hay calificaciones
- Manual de Analisis TransaccionalDocumento147 páginasManual de Analisis TransaccionalAndres Velez100% (4)
- Escroto AgudoDocumento5 páginasEscroto Agudoz. BautistaAún no hay calificaciones
- GLUCONEOGENESISDocumento32 páginasGLUCONEOGENESISzatanna66100% (2)
- Practica CuestionarioDocumento8 páginasPractica CuestionarioJanCarlosPinedoSolanoAún no hay calificaciones
- Diapositivas Turbidimetro NuevaDocumento19 páginasDiapositivas Turbidimetro NuevaLiliveth Martinez GalvanAún no hay calificaciones
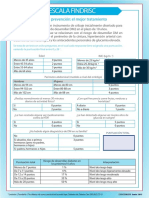
- Escala FindRisc PDFDocumento1 páginaEscala FindRisc PDFAngel Padilla100% (1)
- PTS Desabombe Roca SueltaDocumento3 páginasPTS Desabombe Roca SueltaPachon Robayo Sonita100% (1)
- Desintegración Familiar y ViolenciaDocumento8 páginasDesintegración Familiar y ViolenciaNinaAún no hay calificaciones
- Gastronomía de La Región CaribeDocumento8 páginasGastronomía de La Región CaribeValeri Negrette NuñezAún no hay calificaciones
- INFORME #10 JAGT (Cambio de UF y UEI)Documento3 páginasINFORME #10 JAGT (Cambio de UF y UEI)Maxwell Hardy Cross CastiglianoAún no hay calificaciones
- Diagrama Pespc Cerveza HeinekenDocumento1 páginaDiagrama Pespc Cerveza HeinekenYasaira Lesly Chavez ChavarreyAún no hay calificaciones
- 03.1.2par Gen Car Mor CaroraDocumento8 páginas03.1.2par Gen Car Mor CaroraAmada Zoila Del Carpio RamirezAún no hay calificaciones
- 7 Hierbas para Calmar Los Pensamientos Obsesivos - BelelúDocumento8 páginas7 Hierbas para Calmar Los Pensamientos Obsesivos - BelelújuanfranAún no hay calificaciones
- 1-2019-Biofísica-SILABO-Ego Salazar-1 PDFDocumento14 páginas1-2019-Biofísica-SILABO-Ego Salazar-1 PDFRicardo Simon RojasAún no hay calificaciones
- Nuevos Umbrales de Fe 2Documento132 páginasNuevos Umbrales de Fe 2Luis PerzAún no hay calificaciones
- 6 Labo Control 2 Tejido PlanoDocumento9 páginas6 Labo Control 2 Tejido PlanoJudithMarilynAún no hay calificaciones
- Técnica de La TortugaDocumento3 páginasTécnica de La TortugaEstefany GuerreroAún no hay calificaciones
- CLEAN Manual de LimpiezaDocumento52 páginasCLEAN Manual de Limpiezaandrès martínez krzyzanowskiAún no hay calificaciones
- Copia de Presentación Disfagia CoanilDocumento81 páginasCopia de Presentación Disfagia CoanilLalo LandaAún no hay calificaciones
- Norma Española 13100Documento3 páginasNorma Española 13100Aleksander Segura TinocoAún no hay calificaciones
- Metalurgia Del PlomoDocumento28 páginasMetalurgia Del PlomoSeba Rivano Villagra89% (9)
- Proceso IsobáricoDocumento2 páginasProceso Isobáricomaria0% (1)
- Normas de Referencia - Rev0Documento2 páginasNormas de Referencia - Rev0Victoria MatosAún no hay calificaciones
- Derecho Laboral en VenezuelaDocumento21 páginasDerecho Laboral en VenezuelaMaria AvendanoAún no hay calificaciones
- V.U. Procesadora Avicola de Colombia SAS - Gallina GiganteDocumento2 páginasV.U. Procesadora Avicola de Colombia SAS - Gallina GiganteLina Rocio Rubio RAún no hay calificaciones
- Señalización en GasesDocumento41 páginasSeñalización en GasesGiancarloMlmAún no hay calificaciones
- Espermatología ForenseDocumento25 páginasEspermatología ForenseGuillermo Jesús Haro LázaroAún no hay calificaciones
- Dilemas MoralesDocumento3 páginasDilemas MoralesRichard Antonio Acevedo GutiérrezAún no hay calificaciones
- Catálogo Jugutes Marzo-AbrilDocumento110 páginasCatálogo Jugutes Marzo-AbrilCesar SuarezAún no hay calificaciones