También podría gustarte
- 43691Documento58 páginas43691NelaAún no hay calificaciones
- 43691Documento58 páginas43691NelaAún no hay calificaciones
- MRCP(UK) status in Saudi ArabiaDocumento1 páginaMRCP(UK) status in Saudi ArabiaDrSheika BawazirAún no hay calificaciones
- Peds18 LeukemiaDocumento20 páginasPeds18 LeukemiaDrSheika BawazirAún no hay calificaciones
- Nelson's MCQ'sDocumento150 páginasNelson's MCQ'sDrSheika Bawazir92% (38)
- Cystic Fibrosis 1Documento43 páginasCystic Fibrosis 1DrSheika BawazirAún no hay calificaciones
- School Health Index: A Self-Assessment and Planning GuideDocumento6 páginasSchool Health Index: A Self-Assessment and Planning GuideDrSheika BawazirAún no hay calificaciones
- MCCQE PediatricsDocumento80 páginasMCCQE PediatricsDrSheika Bawazir100% (1)
- عرض تقديميblood donationDocumento25 páginasعرض تقديميblood donationDrSheika BawazirAún no hay calificaciones
- Obstetrics MCQ practice questionsDocumento2 páginasObstetrics MCQ practice questionsDrSheika Bawazir0% (1)
- Perioperative EvaluationDocumento119 páginasPerioperative EvaluationDrSheika BawazirAún no hay calificaciones
- Thoracic Surgery: 5 Year Females of The 3 GroupDocumento69 páginasThoracic Surgery: 5 Year Females of The 3 GroupDrSheika BawazirAún no hay calificaciones
- KAP - of Blood DonationDocumento44 páginasKAP - of Blood DonationDrSheika BawazirAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Malabsorption Seminar: Causes and Nursing CareDocumento42 páginasMalabsorption Seminar: Causes and Nursing CaresomivipinAún no hay calificaciones
- Full Download Nutrition Concepts and Controversies 14th Edition Sizer Solutions ManualDocumento35 páginasFull Download Nutrition Concepts and Controversies 14th Edition Sizer Solutions Manualmarinefeiler540100% (43)
- 1 s2.0 S0929664615003460 MainDocumento7 páginas1 s2.0 S0929664615003460 MainEva GarciaAún no hay calificaciones
- Obu Research Thesise NestleDocumento46 páginasObu Research Thesise NestleHammad Ahmad100% (1)
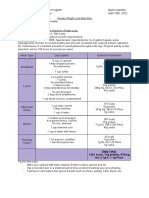
- Obesity Weight Loss Meal PlanDocumento1 páginaObesity Weight Loss Meal Planapi-607536364Aún no hay calificaciones
- Role of Dietary Habits and Diet in CariesDocumento6 páginasRole of Dietary Habits and Diet in CariesȘenchea Crina ElenaAún no hay calificaciones
- How To Create Your Own Self-Sufficient Farm On 4 Acres of LandDocumento44 páginasHow To Create Your Own Self-Sufficient Farm On 4 Acres of LandKevin92% (12)
- The Dnt15: A Shortened Version of The Diabetes Numeracy Test (DNT)Documento13 páginasThe Dnt15: A Shortened Version of The Diabetes Numeracy Test (DNT)zomorda kammounAún no hay calificaciones
- Rajkumar Rao Dentist Alhaurin - ImplantsDocumento4 páginasRajkumar Rao Dentist Alhaurin - ImplantsRajkumar RaoAún no hay calificaciones
- Cdo Foodsphere Inc. San Marino Corned TunaDocumento9 páginasCdo Foodsphere Inc. San Marino Corned TunaCamille Lucelo67% (3)
- Codex General Standard For Food Additives.Documento210 páginasCodex General Standard For Food Additives.Mustafa SehovicAún no hay calificaciones
- Magnesium Verla Product LeafletDocumento3 páginasMagnesium Verla Product LeafletBudi Utami WibawaniAún no hay calificaciones
- Lactation Vegetarian NutritionDocumento2 páginasLactation Vegetarian NutritionFazail SamanyAún no hay calificaciones
- Hippocrates' 7 Levels of HealingDocumento25 páginasHippocrates' 7 Levels of HealingMark Anthony Diego100% (1)
- Natural Bioactive Compounds of Citrus Limon For Food and Health PDFDocumento19 páginasNatural Bioactive Compounds of Citrus Limon For Food and Health PDFEsteban Davila100% (1)
- Nutrition Club FilesDocumento2 páginasNutrition Club FilesRegine SitchonAún no hay calificaciones
- Specialist In Performance Nutrition GuideDocumento24 páginasSpecialist In Performance Nutrition GuidekalikAún no hay calificaciones
- Gant Hybrid Crossfit Strength PDFDocumento21 páginasGant Hybrid Crossfit Strength PDFErgasies KyprosAún no hay calificaciones
- RICKETS and OSTEOGENESIS IMPERFRCTADocumento11 páginasRICKETS and OSTEOGENESIS IMPERFRCTAFaith de la RosaAún no hay calificaciones
- Format C Programs/Programs/Activities: I. Program On IycfDocumento12 páginasFormat C Programs/Programs/Activities: I. Program On IycfKrisna Criselda SimbreAún no hay calificaciones
- Course Outline Nutritional Biochemistry HNDDocumento2 páginasCourse Outline Nutritional Biochemistry HNDMujtabaAún no hay calificaciones
- Clean Diet ExcerptEditionDocumento20 páginasClean Diet ExcerptEditionSusan100% (2)
- Kenneth Saladin - Anatomy & Physiology - The Unity of Form and Function-McGraw-Hill Education (2020) (1) - 1Documento1 páginaKenneth Saladin - Anatomy & Physiology - The Unity of Form and Function-McGraw-Hill Education (2020) (1) - 1Guilherme RodriguesAún no hay calificaciones
- Pasacao Town Holds 1St Tourism Summit: New Camsur PNP Director Assumes PostDocumento8 páginasPasacao Town Holds 1St Tourism Summit: New Camsur PNP Director Assumes PostBikol ReporterAún no hay calificaciones
- Freezing Fresh Fruits: Before Packaging Types of PacksDocumento8 páginasFreezing Fresh Fruits: Before Packaging Types of PacksgkreddiAún no hay calificaciones
- Code of Ethics For DietitiansDocumento12 páginasCode of Ethics For DietitiansScarletAún no hay calificaciones
- Essential Nutrition The BookDocumento115 páginasEssential Nutrition The BookTron2009Aún no hay calificaciones
- Unilever Management ProjectDocumento34 páginasUnilever Management ProjectAamir Raza75% (4)
- Mizoram Civil Services (Combined Competitive Examination) Updated (14th May 2012) - 2 PDFDocumento96 páginasMizoram Civil Services (Combined Competitive Examination) Updated (14th May 2012) - 2 PDFsangasangteaAún no hay calificaciones
- DR Renaud BrochureDocumento15 páginasDR Renaud BrochureNazihCosmetics0% (1)