También podría gustarte
- 76 Cheat Sheets For Nursing StudentsDocumento95 páginas76 Cheat Sheets For Nursing StudentsIly Lagoniya100% (14)
- Stroke Topic DiscussionDocumento19 páginasStroke Topic Discussionapi-648714317Aún no hay calificaciones
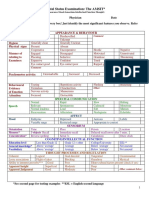
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocumento2 páginasMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- 1 s2.0 S0735109716366992 mmc1Documento10 páginas1 s2.0 S0735109716366992 mmc1Pangala NitaAún no hay calificaciones
- 1 s2.0 S0735109716366992 mmc1Documento8 páginas1 s2.0 S0735109716366992 mmc1Pangala NitaAún no hay calificaciones
- William C. Cushman, MD, FACP, FAHA: Veterans Affairs Medical Center, Memphis, TN For The ACCORD Study GroupDocumento24 páginasWilliam C. Cushman, MD, FACP, FAHA: Veterans Affairs Medical Center, Memphis, TN For The ACCORD Study GroupCardiologyNetwork.comAún no hay calificaciones
- Statins in CVD Management: Is Just Lipid Lowering Enough?Documento37 páginasStatins in CVD Management: Is Just Lipid Lowering Enough?SriAún no hay calificaciones
- Atorvastatin Statin in CVD ManagementDocumento37 páginasAtorvastatin Statin in CVD ManagementSriAún no hay calificaciones
- Management of Hypertension and Dyslipidemia in 2016: Key Updates from Recent GuidelinesDocumento27 páginasManagement of Hypertension and Dyslipidemia in 2016: Key Updates from Recent GuidelinesSinta ChoiAún no hay calificaciones
- Eddy Wirawan, SPJP - Fiha: Rsud. Ulin BanjarmasinDocumento49 páginasEddy Wirawan, SPJP - Fiha: Rsud. Ulin Banjarmasineka febriantyAún no hay calificaciones
- Cerebrovascular Diseases: Global Burden and Prevention StrategiesDocumento28 páginasCerebrovascular Diseases: Global Burden and Prevention StrategiesbagussofianAún no hay calificaciones
- Antiplatelet and Anticoagulation GuideDocumento31 páginasAntiplatelet and Anticoagulation GuideMarcelliaAún no hay calificaciones
- Ehf2 7 1125Documento5 páginasEhf2 7 1125Pranvera ApostoliAún no hay calificaciones
- Pengelolaan Hipertensi: Fajar YuwantoDocumento37 páginasPengelolaan Hipertensi: Fajar YuwantoPutri Ria AriyantiAún no hay calificaciones
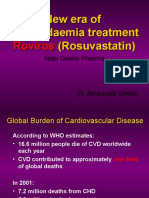
- RosuvastatinDocumento62 páginasRosuvastatinEileen del RosarioAún no hay calificaciones
- 6 Studii StatineDocumento37 páginas6 Studii Statinejust4uhopeAún no hay calificaciones
- The Results of The Study of Heart and Renal Protection (SHARP)Documento19 páginasThe Results of The Study of Heart and Renal Protection (SHARP)Surya MahardikaAún no hay calificaciones
- Catalano1992 PDFDocumento6 páginasCatalano1992 PDFSepti Fadhilah SPAún no hay calificaciones
- Treatment of Hypertension: Jai Radhakrishnan, M.D. Division of NephrologyDocumento34 páginasTreatment of Hypertension: Jai Radhakrishnan, M.D. Division of NephrologyAndika HAún no hay calificaciones
- 15 Advance TrialDocumento35 páginas15 Advance TrialShaheen UsmaniAún no hay calificaciones
- CASE PRESENTATION ON U AnginaDocumento40 páginasCASE PRESENTATION ON U AnginaSafoora RafeeqAún no hay calificaciones
- 980517 Dr 血液透析訓練班Documento64 páginas980517 Dr 血液透析訓練班amalAún no hay calificaciones
- Treatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlideDocumento31 páginasTreatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlidejoshuaAún no hay calificaciones
- Systolic Blood Pressure Intervention Trial (SPRINT) Principal ResultsDocumento31 páginasSystolic Blood Pressure Intervention Trial (SPRINT) Principal ResultsAdellia Risda SativaAún no hay calificaciones
- Long-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyDocumento22 páginasLong-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyFlore HountondjiAún no hay calificaciones
- HopeDocumento21 páginasHopeIsnawan WidyayantoAún no hay calificaciones
- antiHIPERTENSI 2020Documento88 páginasantiHIPERTENSI 2020nabila fikriAún no hay calificaciones
- Antagonis Reseptor Angiotensin 2, AIIRADocumento31 páginasAntagonis Reseptor Angiotensin 2, AIIRAsuho exoAún no hay calificaciones
- Clinical Study Report: Prevalence of Peripheral Arterial Disease in Acute Coronary Syndrome PatientsDocumento5 páginasClinical Study Report: Prevalence of Peripheral Arterial Disease in Acute Coronary Syndrome PatientsFlavius Ion NicolaeAún no hay calificaciones
- Ascot BplaDocumento12 páginasAscot BplaMelissa DelgadoAún no hay calificaciones
- Global Risk of Cardiovascular Disease: Assessment and ApplicationDocumento18 páginasGlobal Risk of Cardiovascular Disease: Assessment and ApplicationEmdan SengadjiAún no hay calificaciones
- Morning Report: Dr. Dikara WS Maulidy, SP - PDDocumento24 páginasMorning Report: Dr. Dikara WS Maulidy, SP - PDBethari Abi SafitriAún no hay calificaciones
- Updated Hypertension GuidelineDocumento88 páginasUpdated Hypertension Guidelinekenny631653Aún no hay calificaciones
- Case PresentationDocumento5 páginasCase PresentationMeriska AhmadAún no hay calificaciones
- Lipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeDocumento65 páginasLipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeRoby KieranAún no hay calificaciones
- Hypertension LectureDocumento105 páginasHypertension LectureSnigdha GomberAún no hay calificaciones
- Tutorial Hipertensi IiDocumento34 páginasTutorial Hipertensi Iikemuning nasutionAún no hay calificaciones
- Pengelolaan Hipertensi: Fajar Yuwanto SMF Penyakit Dalam RS Abdul MoeloekDocumento45 páginasPengelolaan Hipertensi: Fajar Yuwanto SMF Penyakit Dalam RS Abdul MoeloekJovankaAún no hay calificaciones
- JurnalDocumento5 páginasJurnalKardio JuliAún no hay calificaciones
- Salisbury 1100 Harrison PDFDocumento62 páginasSalisbury 1100 Harrison PDFDrNaveen Singh Rajpurohit KaduAún no hay calificaciones
- Management of CAD: Role of Beta BlockerDocumento89 páginasManagement of CAD: Role of Beta BlockerPragnesh ShahAún no hay calificaciones
- How Should One Decide Whom To Treat For Hypertension?: Jay N. Cohn, M.DDocumento33 páginasHow Should One Decide Whom To Treat For Hypertension?: Jay N. Cohn, M.DAn-Nisa Khoirun UmmiAún no hay calificaciones
- How To Control BP (BPJS MLG 14 Okt 2014) DR AtmaDocumento62 páginasHow To Control BP (BPJS MLG 14 Okt 2014) DR AtmaaceAún no hay calificaciones
- Habits Vs Evidence RAAS ARB Talk FinalDocumento45 páginasHabits Vs Evidence RAAS ARB Talk Finalswaleh breik misfirAún no hay calificaciones
- Case Report on 48-Year-Old Female with Right Hemiparesis and AphasiaDocumento41 páginasCase Report on 48-Year-Old Female with Right Hemiparesis and AphasiaSabella Gustika VernandaAún no hay calificaciones
- Yashwanth - IHD HFrEfDocumento16 páginasYashwanth - IHD HFrEfYashwanth N BAún no hay calificaciones
- STEMI Inferior Wall Onset 3 Hours Killip I: Dr. Juzny Alkatiri, SP - PD, SP - JP, Fiha, FinasimDocumento33 páginasSTEMI Inferior Wall Onset 3 Hours Killip I: Dr. Juzny Alkatiri, SP - PD, SP - JP, Fiha, FinasimAnwar Mo SajaAún no hay calificaciones
- Clinical Study Report: Prevalence of Peripheral Arterial Disease in Acute Coronary Syndrome PatientsDocumento4 páginasClinical Study Report: Prevalence of Peripheral Arterial Disease in Acute Coronary Syndrome PatientsRadu AnaAún no hay calificaciones
- Renalised HypertensionDocumento43 páginasRenalised HypertensionsuganAún no hay calificaciones
- Responsi Stemi Dr. Tuko SP - JP FixDocumento56 páginasResponsi Stemi Dr. Tuko SP - JP FixcintaAún no hay calificaciones
- K 3a HipertensiDocumento42 páginasK 3a HipertensithalamusAún no hay calificaciones
- Materi Hipertensi Dr. Irma W, SP - PDDocumento56 páginasMateri Hipertensi Dr. Irma W, SP - PDFina Syahrotul AdzimahAún no hay calificaciones
- FinalReport ModelStudentiDocumento5 páginasFinalReport ModelStudentiTeodor BuseAún no hay calificaciones
- Exanple Re-Ly-Trial-DabigatranDocumento5 páginasExanple Re-Ly-Trial-DabigatranPollaRxsu RuenroengboonAún no hay calificaciones
- Cardiology Department Dustira District Hospital Faculty of Medicine Tanjungpura University 2018Documento11 páginasCardiology Department Dustira District Hospital Faculty of Medicine Tanjungpura University 2018Destri R.Aún no hay calificaciones
- Approach to Thrombophilia (1)Documento58 páginasApproach to Thrombophilia (1)Vanessa EdizaAún no hay calificaciones
- hypertension final PDFDocumento48 páginashypertension final PDFakshayshinde24995Aún no hay calificaciones
- Thyroid StormDocumento35 páginasThyroid StormZulfanaAún no hay calificaciones
- Antihypertensive in Preeclampsia - Prof. SarmaDocumento34 páginasAntihypertensive in Preeclampsia - Prof. SarmaFellita Ratri AAún no hay calificaciones
- JNC 8: What changes may be in store for hypertension guidelinesDocumento47 páginasJNC 8: What changes may be in store for hypertension guidelinesDavid Chandra EriksonAún no hay calificaciones
- Cardiac Care and COVID-19: Perspectives in Medical PracticeDe EverandCardiac Care and COVID-19: Perspectives in Medical PracticeAún no hay calificaciones
- E A R D o C 2010 InvDocumento16 páginasE A R D o C 2010 InvBarak ShitritAún no hay calificaciones
- Jurnal Pendukung 2Documento13 páginasJurnal Pendukung 2Eko PrasAún no hay calificaciones
- Intersect ENT Investor Presentation - $XENTDocumento28 páginasIntersect ENT Investor Presentation - $XENTmedtechyAún no hay calificaciones
- Psychiatric and Mental Health NursingDocumento10 páginasPsychiatric and Mental Health NursingGlaiza Claire Am-amlan OlayanAún no hay calificaciones
- Rectal ProlapseDocumento2 páginasRectal ProlapseSalem ZoghbyAún no hay calificaciones
- Freud, Unconscious ExplorerDocumento5 páginasFreud, Unconscious ExplorerRyder Blue Holmes WilsonAún no hay calificaciones
- October 2017 Ophthalmic PearlsDocumento3 páginasOctober 2017 Ophthalmic PearlsShafa KhansaAún no hay calificaciones
- Aiswarya Krishna: Professional SummaryDocumento4 páginasAiswarya Krishna: Professional SummaryRejoy RadhakrishnanAún no hay calificaciones
- Maternal Pulse Pressure and The Risk of Postepidural ComplicationsDocumento11 páginasMaternal Pulse Pressure and The Risk of Postepidural ComplicationsRiany Jade SabrinaAún no hay calificaciones
- Jurnal Kesehatan: Analisis Waste Dengan Model Lean Hospital Pada Pelayanan Poli Rawat JalanDocumento10 páginasJurnal Kesehatan: Analisis Waste Dengan Model Lean Hospital Pada Pelayanan Poli Rawat JalanGuillermo Luis AcostaAún no hay calificaciones
- Reporting and Learning Systems for Medication ErrorsDocumento7 páginasReporting and Learning Systems for Medication ErrorsNoor KevAún no hay calificaciones
- Dental Caries IndexDocumento35 páginasDental Caries Indexdr parveen bathla100% (1)
- Distalization of Maxillary Molars Using A Lever Arm and Mini-ImplantDocumento10 páginasDistalization of Maxillary Molars Using A Lever Arm and Mini-ImplantYury Tenorio CahuanaAún no hay calificaciones
- Week 1 MCQ VMPFDocumento25 páginasWeek 1 MCQ VMPFZainab_Wajih_2544100% (1)
- Weebly ResumeDocumento4 páginasWeebly Resumeapi-295640482Aún no hay calificaciones
- Aseptic Non Touch Technique - A Guide For Healthcare WorkersDocumento2 páginasAseptic Non Touch Technique - A Guide For Healthcare Workersananda apryliaAún no hay calificaciones
- PTSD Treatment ManualDocumento54 páginasPTSD Treatment Manualdrjchandler100% (4)
- HPPDocumento1 páginaHPPMuhammad FadzrulAún no hay calificaciones
- Fitz Cardiology Paces NotesDocumento26 páginasFitz Cardiology Paces NotesMuhammad BilalAún no hay calificaciones
- Safe Blood UseDocumento2 páginasSafe Blood UseAnnette LowryAún no hay calificaciones
- Er LFD 11Documento1 páginaEr LFD 11EldwinCauilanAún no hay calificaciones
- Application CoopMED Health Insurance Plan BarbadosDocumento2 páginasApplication CoopMED Health Insurance Plan BarbadosKammieAún no hay calificaciones
- Clinical Characteristics of Raoultella Ornithinolytica BacteremiaDocumento6 páginasClinical Characteristics of Raoultella Ornithinolytica BacteremiaEnrique MartínezAún no hay calificaciones
- Survival Strategies For Parenting The Child & Teen With BipolarDocumento236 páginasSurvival Strategies For Parenting The Child & Teen With Bipolarseptiadhi wirawanAún no hay calificaciones
- Early Enteral NutritionDocumento55 páginasEarly Enteral NutritionAdya ArradikhaAún no hay calificaciones
- Short Sightedness Vs Long SightDocumento1 páginaShort Sightedness Vs Long SightDevill DavajAún no hay calificaciones
- Aapd Guidelines - Restorative DentistryDocumento8 páginasAapd Guidelines - Restorative DentistrymahmoudAún no hay calificaciones
- 4.megaloblastik AnemiaDocumento16 páginas4.megaloblastik AnemiahadiemAún no hay calificaciones
- Acceptance of Dying A Discourse Analysis of Palliative Care LiteratureDocumento8 páginasAcceptance of Dying A Discourse Analysis of Palliative Care LiteratureMauricio MartinezAún no hay calificaciones