También podría gustarte
- Colorectal Surgery: Clinical Care and ManagementDe EverandColorectal Surgery: Clinical Care and ManagementBruce GeorgeAún no hay calificaciones
- LiverDocumento167 páginasLiverWai Kwong ChiuAún no hay calificaciones
- 5th Year Git LectureDocumento75 páginas5th Year Git Lecturekasilat574Aún no hay calificaciones
- Transplant Liver Imaging PresentationDocumento48 páginasTransplant Liver Imaging PresentationChristopher MejiasAún no hay calificaciones
- Lecture09 Radiological Examination of The Liver, Biliary Tract and PancreasDocumento56 páginasLecture09 Radiological Examination of The Liver, Biliary Tract and PancreassinisarAún no hay calificaciones
- Imaging in Small Bowel Tumors: Dr. Muhammad Bin Zulfiqar Pgr-Iii Fcps Sims/ShlDocumento60 páginasImaging in Small Bowel Tumors: Dr. Muhammad Bin Zulfiqar Pgr-Iii Fcps Sims/ShlDdfdf sdfAún no hay calificaciones
- Urinary Tract TumourDocumento40 páginasUrinary Tract TumourNu JoeAún no hay calificaciones
- Wilms Tumor Hank Baskin, MDDocumento11 páginasWilms Tumor Hank Baskin, MDPraktekDokterMelatiAún no hay calificaciones
- LIVER MassesDocumento3 páginasLIVER MassesDaniel MontesAún no hay calificaciones
- Hepatocellularcarcinoma Andotherhepatic Malignancies:: MR ImagingDocumento25 páginasHepatocellularcarcinoma Andotherhepatic Malignancies:: MR ImagingJOSE LIZANDRO SOPLAPUCO RUIZAún no hay calificaciones
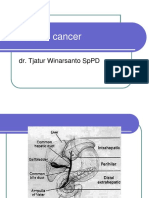
- Pancreatic Cancer: Dr. Tjatur Winarsanto SPPDDocumento41 páginasPancreatic Cancer: Dr. Tjatur Winarsanto SPPDMayiz Renata LimerseAún no hay calificaciones
- EAU Pocket On Renal Cell Carcinoma 2024Documento35 páginasEAU Pocket On Renal Cell Carcinoma 2024nadaelhaousAún no hay calificaciones
- Radiology of Hepatobiliary System Pancreas and Spleen: Nugzar LipartelianiDocumento136 páginasRadiology of Hepatobiliary System Pancreas and Spleen: Nugzar LipartelianiShubham TanwarAún no hay calificaciones
- Neoplasms of The Genitourinary TractDocumento71 páginasNeoplasms of The Genitourinary Tractvishalzenia100% (2)
- Imaging Hepatobiliary DanzDocumento71 páginasImaging Hepatobiliary DanzIntanAún no hay calificaciones
- Liver TumoursDocumento37 páginasLiver TumoursChenuri RanasingheAún no hay calificaciones
- Liver Disease: Schwartz Principles of Surgery2010Documento50 páginasLiver Disease: Schwartz Principles of Surgery2010ralphAún no hay calificaciones
- Cellular Aberration Reviewer 5-6Documento9 páginasCellular Aberration Reviewer 5-6Jessica A. BurgosAún no hay calificaciones
- Salivary TumorDocumento54 páginasSalivary TumorPartha GanesanAún no hay calificaciones
- Liver CancerDocumento44 páginasLiver CancerJoyce Ann CumlatAún no hay calificaciones
- Cholangiocarcinoma: R.KarthikeyanDocumento49 páginasCholangiocarcinoma: R.KarthikeyanKarthikeyan R100% (2)
- Renal Tumors: DR. Mohamed ElgendyDocumento27 páginasRenal Tumors: DR. Mohamed ElgendyDani DanyAún no hay calificaciones
- Imaging Hepatobiliary DanzDocumento74 páginasImaging Hepatobiliary DanzArio Lukas100% (1)
- MNGT of Renal Tumors-2Documento66 páginasMNGT of Renal Tumors-2Tsega WesenAún no hay calificaciones
- Liver CancerDocumento44 páginasLiver CancerEjay Jacob Ricamara50% (2)
- O Develop Either Into Hepatocytes or Intrahepatic Ductal CellsDocumento10 páginasO Develop Either Into Hepatocytes or Intrahepatic Ductal CellsClint MorrisonAún no hay calificaciones
- Colorectal Cancer: - Dr. Suneet KhuranaDocumento36 páginasColorectal Cancer: - Dr. Suneet KhuranaCarlo ToledooAún no hay calificaciones
- General Guidelines For CT ProtocolsDocumento4 páginasGeneral Guidelines For CT ProtocolsBilal Maqsood SukheraAún no hay calificaciones
- M. Ali Asdar Departement of Pulmonology and Respiratory Medicine Faculty of Medicine University of Indonesia - Persahabatan General Hospital JakartaDocumento30 páginasM. Ali Asdar Departement of Pulmonology and Respiratory Medicine Faculty of Medicine University of Indonesia - Persahabatan General Hospital JakartaAsdar AsjunoAún no hay calificaciones
- Cystic Focal Liver Lesions in The Adult: Differential CT and MR Imaging FeaturesDocumento35 páginasCystic Focal Liver Lesions in The Adult: Differential CT and MR Imaging FeaturesRazan AlayedAún no hay calificaciones
- Liver Tumors BasicDocumento37 páginasLiver Tumors BasicIrene Zae MwandotoAún no hay calificaciones
- Renal Cell CarcinomaDocumento10 páginasRenal Cell Carcinoma'asyura Mohd RezaAún no hay calificaciones
- Liver TumorsDocumento52 páginasLiver TumorsRajendra DesaiAún no hay calificaciones
- Renal NeoplasmDocumento153 páginasRenal NeoplasmTHESSNAVARRO100% (2)
- Bladder Cancer 2021Documento30 páginasBladder Cancer 2021MAD Bl00DAún no hay calificaciones
- Surgery - Oral ExamDocumento37 páginasSurgery - Oral ExamShidev100% (1)
- Liver Review: Dr. Ahmed Kandil, MD, Phd. Consultant Surgeon Head of Surgery Department Shifa Hosp. - GazaDocumento76 páginasLiver Review: Dr. Ahmed Kandil, MD, Phd. Consultant Surgeon Head of Surgery Department Shifa Hosp. - GazaMukherjeeNityanandaAún no hay calificaciones
- EAU Pocket On Renal Cell Carcinoma 2023Documento29 páginasEAU Pocket On Renal Cell Carcinoma 2023Phuoc LeAún no hay calificaciones
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocumento83 páginasDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudAún no hay calificaciones
- Hepatocellular Carcinoma - Diagnosis and TreatmentDocumento46 páginasHepatocellular Carcinoma - Diagnosis and TreatmentSigh BalaAún no hay calificaciones
- Rectosigmoid Cancer: Block 8B Sacdalan To SengaDocumento58 páginasRectosigmoid Cancer: Block 8B Sacdalan To SengaAngeli-Tristel SaquitanAún no hay calificaciones
- EAU Pocket On Renal Cell Carcinoma 2022Documento28 páginasEAU Pocket On Renal Cell Carcinoma 2022Dane QhAún no hay calificaciones
- History History: Past Medical History: Past Medical HistoryDocumento7 páginasHistory History: Past Medical History: Past Medical HistoryAtandi JosephatAún no hay calificaciones
- Pancreatic CancerDocumento25 páginasPancreatic CancerAatir JavaidAún no hay calificaciones
- Carcinoma of OesophagusDocumento18 páginasCarcinoma of Oesophaguszxcvbzaki123Aún no hay calificaciones
- L1 Radiology 2Documento55 páginasL1 Radiology 2Princess FAún no hay calificaciones
- Flank PainDocumento9 páginasFlank PainMuhammad HassanAún no hay calificaciones
- Traumatic Abdomen FinalDocumento162 páginasTraumatic Abdomen FinalCandice LavigneAún no hay calificaciones
- HEPATOMADocumento30 páginasHEPATOMASemestaAún no hay calificaciones
- Urology SummaryDocumento33 páginasUrology Summarylalo5eerAún no hay calificaciones
- EAU 2024 Pocket GuidelinesDocumento571 páginasEAU 2024 Pocket Guidelinesgreatkhanjee82Aún no hay calificaciones
- Liver Study MaterialDocumento17 páginasLiver Study MaterialRazan AlayedAún no hay calificaciones
- Colorectal CancerDocumento31 páginasColorectal CancerIrene RealinoAún no hay calificaciones
- Liver Cancer Oncologic NursingDocumento28 páginasLiver Cancer Oncologic NursingMari ManlapazAún no hay calificaciones
- Tumor Thrombus: Incidence, Imaging, Prognosis and TreatmentDocumento13 páginasTumor Thrombus: Incidence, Imaging, Prognosis and TreatmentDuccio RossiAún no hay calificaciones
- Cholangiocarcinoma - Radiology Reference Article - RadiopaediaDocumento5 páginasCholangiocarcinoma - Radiology Reference Article - RadiopaediaWill SmithAún no hay calificaciones
- Colorectal Ca (CRC) .: Malueth Abraham, MBCHB ViDocumento36 páginasColorectal Ca (CRC) .: Malueth Abraham, MBCHB ViMalueth AnguiAún no hay calificaciones
- Urology Sub Division Department of Surgery Medical School University of Sumatera UtaraDocumento34 páginasUrology Sub Division Department of Surgery Medical School University of Sumatera UtaraenriAún no hay calificaciones
- Primary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportDocumento6 páginasPrimary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportRais KhairuddinAún no hay calificaciones
- Testicular CancerDocumento24 páginasTesticular CancerJulianne LeeAún no hay calificaciones
- Xrays, MRI ActivitiesDocumento2 páginasXrays, MRI Activitiessokhna.sall.545Aún no hay calificaciones
- TocOSCE PediatricsDocumento14 páginasTocOSCE Pediatricssamy22722Aún no hay calificaciones
- Mobile Mobile Radiography Radiography Gpy GpyDocumento10 páginasMobile Mobile Radiography Radiography Gpy GpyPaulAún no hay calificaciones
- Hospital TeamDocumento2 páginasHospital TeamSelimatulAún no hay calificaciones
- CT Pulmonary AngiographyDocumento7 páginasCT Pulmonary AngiographydanielageorgianaAún no hay calificaciones
- Launching A Healthcare Program SampleDocumento35 páginasLaunching A Healthcare Program SampleRonald LlacunaAún no hay calificaciones
- ECR2019 Final Programme Web FINAL 190214Documento446 páginasECR2019 Final Programme Web FINAL 190214Manuel CalvoAún no hay calificaciones
- LHU RAD UMUM Toshiba RS Kurnia CilegonDocumento20 páginasLHU RAD UMUM Toshiba RS Kurnia CilegonDwi FatmawatiAún no hay calificaciones
- Siemens Cios FusionDocumento23 páginasSiemens Cios FusionEldane Grace PontinoAún no hay calificaciones
- Transcranial Doppler Ultrasound Examination For Adults and ChildrenDocumento12 páginasTranscranial Doppler Ultrasound Examination For Adults and ChildrenJuan José Ruiz CastilloAún no hay calificaciones
- Chest & Abdomen Mobile Radiography - DR - RanaDocumento23 páginasChest & Abdomen Mobile Radiography - DR - RanaRana Abd AlmugeethAún no hay calificaciones
- Antony Paull J: ObjectiveDocumento5 páginasAntony Paull J: ObjectivefreedaAún no hay calificaciones
- Art 3A10.1007 2Fs00259 013 2535 3 PDFDocumento477 páginasArt 3A10.1007 2Fs00259 013 2535 3 PDFHerryAsu-songkoAún no hay calificaciones
- Agfa CR85-X Mammogreaphy PDFDocumento28 páginasAgfa CR85-X Mammogreaphy PDFNasr Eldin AlyAún no hay calificaciones
- Guidelines For The Use of Digital Detector Arrays and Computed Radiology For Aerospace Casting InspectionsDocumento32 páginasGuidelines For The Use of Digital Detector Arrays and Computed Radiology For Aerospace Casting InspectionsFabien Faucher100% (2)
- Prelim Physio PsychDocumento28 páginasPrelim Physio PsychRM April AlonAún no hay calificaciones
- Case Presentation - Iort Breast CancerDocumento25 páginasCase Presentation - Iort Breast Cancerapi-498552797Aún no hay calificaciones
- 50 Imaging Studies Every Doctor Should KnowDocumento353 páginas50 Imaging Studies Every Doctor Should KnowYokoAún no hay calificaciones
- Lra 181458 Non Operating Room Anesthesia Patient Selection and SpecialDocumento9 páginasLra 181458 Non Operating Room Anesthesia Patient Selection and SpecialEric Aguilar SantiagoAún no hay calificaciones
- (ZEN-7000) User's Manual Eng Ver2.1 - CE 2460Documento64 páginas(ZEN-7000) User's Manual Eng Ver2.1 - CE 2460Gauss Medikal Sistemler100% (1)
- U L S E C - Usls Bl1-P: Ltrasound IFE Upport Ntry OurseDocumento9 páginasU L S E C - Usls Bl1-P: Ltrasound IFE Upport Ntry Oursesaraswaty710Aún no hay calificaciones
- NCRP Report No. 177 PDFDocumento245 páginasNCRP Report No. 177 PDFVivien FerradaAún no hay calificaciones
- The Clinical Impact of Volumetric and Helical CT ImagingDocumento12 páginasThe Clinical Impact of Volumetric and Helical CT ImagingAndre ClouatreAún no hay calificaciones
- Histopathologic Analysis of Ct-Guided Core Needle Biopsy in Radiologically Detected Suspicious Mediastinal and Lung Mass: Two Years' Study in Tertiary HospitalDocumento4 páginasHistopathologic Analysis of Ct-Guided Core Needle Biopsy in Radiologically Detected Suspicious Mediastinal and Lung Mass: Two Years' Study in Tertiary HospitalDesiree MejicaAún no hay calificaciones
- Cherry Hill 1106Documento24 páginasCherry Hill 1106elauwitAún no hay calificaciones
- Shs - NarrativeDocumento74 páginasShs - NarrativeMercado MinaAún no hay calificaciones
- RadiologyDocumento1 páginaRadiologyKaran AroraAún no hay calificaciones
- Review Jurnal RadiologiDocumento10 páginasReview Jurnal RadiologiM Benni KadapihAún no hay calificaciones
- Contrast MediaDocumento6 páginasContrast MediardmdelarosaAún no hay calificaciones
- Somatom Definition Edge Brochure-00024835Documento56 páginasSomatom Definition Edge Brochure-00024835manuel pilco riosAún no hay calificaciones