También podría gustarte
- Primary Amenorrhoea 2Documento42 páginasPrimary Amenorrhoea 2sivaAún no hay calificaciones
- Clinical Guidelines ForDocumento54 páginasClinical Guidelines ForHenry SudharsonoAún no hay calificaciones
- 2 AmenorrheaDocumento41 páginas2 AmenorrheaKilp MosesAún no hay calificaciones
- AmenorrheaDocumento55 páginasAmenorrheaAla AbushehabAún no hay calificaciones
- 3 AmenorrrheaDocumento29 páginas3 AmenorrrheaKilp MosesAún no hay calificaciones
- Amennorhoea Dinu PDFDocumento11 páginasAmennorhoea Dinu PDFprabuddhiAún no hay calificaciones
- Amen or RheaDocumento41 páginasAmen or Rheakhadzx100% (2)
- AmenorrheaDocumento41 páginasAmenorrheaBonitavanyAún no hay calificaciones
- 4.4 (Amenorrhea) University of AlexanderDocumento28 páginas4.4 (Amenorrhea) University of AlexanderAnonymous XSXlZJvyWAún no hay calificaciones
- Amenorrhoea: 8 Semester ROLL NO: 90, 91, 92, 93, 94Documento69 páginasAmenorrhoea: 8 Semester ROLL NO: 90, 91, 92, 93, 94Sharoon KumarAún no hay calificaciones
- 4.primary - Secondary AmenorrheaDocumento5 páginas4.primary - Secondary AmenorrheaAhmed Al GhaithiAún no hay calificaciones
- Dr. Shehla Jamal Assistant Professor: OBG S M S & RDocumento69 páginasDr. Shehla Jamal Assistant Professor: OBG S M S & RAppy LoveAún no hay calificaciones
- Amenorrhea - DrPrekshyaDocumento44 páginasAmenorrhea - DrPrekshyaasdfAún no hay calificaciones
- من دون عنوانDocumento50 páginasمن دون عنوانjjeddawAún no hay calificaciones
- Primary Amenorrhea: Rabika Almina RabiaDocumento30 páginasPrimary Amenorrhea: Rabika Almina RabiaAlmina RehmanAún no hay calificaciones
- Menstrual DisordersDocumento29 páginasMenstrual DisorderstuhinsinghAún no hay calificaciones
- Amenorrhea: An-Najah National University DR - Ahmad Abu KhaizaranDocumento26 páginasAmenorrhea: An-Najah National University DR - Ahmad Abu KhaizaranZyad MadiAún no hay calificaciones
- MEETING 6 AmenorrheaDocumento41 páginasMEETING 6 AmenorrheaNader KhouryAún no hay calificaciones
- Absence of A Menstrual PeriodDocumento2 páginasAbsence of A Menstrual PeriodDragan PetrovicAún no hay calificaciones
- AmenorrheaDocumento23 páginasAmenorrheaKarmmanya Razahani PurnamaAún no hay calificaciones
- AmenorrheaDocumento41 páginasAmenorrheadoraAún no hay calificaciones
- Amennorhea Summary in A TableDocumento3 páginasAmennorhea Summary in A TableAmalia GeorgiouAún no hay calificaciones
- AmenorrheaDocumento41 páginasAmenorrheaDewi Felayati Gusni100% (2)
- Secondaryamenorrhoealectures 230316163724 360b79b3Documento42 páginasSecondaryamenorrhoealectures 230316163724 360b79b3droc ahmedAún no hay calificaciones
- Obstetrics & Gynecology: Original Review & Revision HyderabadDocumento739 páginasObstetrics & Gynecology: Original Review & Revision Hyderabad24k.avinashAún no hay calificaciones
- AmenorrhoeaDocumento38 páginasAmenorrhoeaheydydAún no hay calificaciones
- Amenorrhea, Hirsutism & Polycystic Ovary SyndromeDocumento15 páginasAmenorrhea, Hirsutism & Polycystic Ovary SyndromeSecret ManAún no hay calificaciones
- Gannguan PubertasDocumento56 páginasGannguan PubertasAde Yosdi PutraAún no hay calificaciones
- AmenorrheaDocumento41 páginasAmenorrheaarfahregarAún no hay calificaciones
- Amenorrhoea 5thyr DR KKDocumento56 páginasAmenorrhoea 5thyr DR KKpmj050gpAún no hay calificaciones
- AMENORRHEADocumento6 páginasAMENORRHEAChristian PasicolanAún no hay calificaciones
- AMENORRHOEADocumento16 páginasAMENORRHOEAdrravindermehetreyAún no hay calificaciones
- Mission Fmge Obg Day-6 - 231114 - 215211Documento137 páginasMission Fmge Obg Day-6 - 231114 - 215211CastleKGAún no hay calificaciones
- Rps138 Slide AmenorrheaDocumento41 páginasRps138 Slide Amenorrheasyahidah nadiahAún no hay calificaciones
- AmenorrheaDocumento56 páginasAmenorrheaMrTriumphantAún no hay calificaciones
- Amenorrhea - Algorithm & DifferentialsDocumento9 páginasAmenorrhea - Algorithm & DifferentialsItharshan IndreswaranAún no hay calificaciones
- First Aid For The OBS&GYN Clerkship CH 17 (Amenorrhea)Documento9 páginasFirst Aid For The OBS&GYN Clerkship CH 17 (Amenorrhea)黃芳昌Aún no hay calificaciones
- Sexual Differentiation Anomalies+Puberty - PPT Fara PozeDocumento49 páginasSexual Differentiation Anomalies+Puberty - PPT Fara PozeAmira AsaadAún no hay calificaciones
- Sexuality and IntersexualityDocumento23 páginasSexuality and IntersexualityManu BharadwazAún no hay calificaciones
- Amenorrhea: DR - Muhammad Rusda, SP - OG (K)Documento41 páginasAmenorrhea: DR - Muhammad Rusda, SP - OG (K)sridhaniAún no hay calificaciones
- AmenorrheaDocumento51 páginasAmenorrheaAyalewAún no hay calificaciones
- Homoeopathic Management of InfertilityDocumento92 páginasHomoeopathic Management of InfertilityDrSaji86% (7)
- Secondary Amenorrhea: DR Hanaa AlaniDocumento44 páginasSecondary Amenorrhea: DR Hanaa AlaniAakashAún no hay calificaciones
- Amenorhea 2023Documento18 páginasAmenorhea 2023S HelAún no hay calificaciones
- Amenorrhea PDFDocumento5 páginasAmenorrhea PDFKenneth Robin CarbonellAún no hay calificaciones
- IntersexnnDocumento66 páginasIntersexnnSyahputraWibowoAún no hay calificaciones
- Gynae 1Documento3 páginasGynae 1Gokul DevAún no hay calificaciones
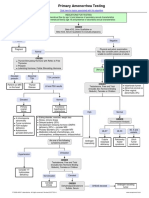
- Primary Amenorrhea Testing AlgorithmDocumento1 páginaPrimary Amenorrhea Testing AlgorithmfarmasiAún no hay calificaciones
- Primary Amenorrhea Testing AlgorithmDocumento1 páginaPrimary Amenorrhea Testing AlgorithmGabriella AguirreAún no hay calificaciones
- Disorders of Growth and DevelopmentDocumento52 páginasDisorders of Growth and DevelopmentMaria Hudson100% (1)
- Secondary Amenorrhea: District I ACOG Medical Student Education Module 2009Documento18 páginasSecondary Amenorrhea: District I ACOG Medical Student Education Module 2009Anca Berescu StefanAún no hay calificaciones
- EndokrinDocumento65 páginasEndokrinZulia Ahmad BurhaniAún no hay calificaciones
- Chapter 5 AmenorrhoeaDocumento7 páginasChapter 5 Amenorrhoeapmj050gpAún no hay calificaciones
- Infertility 001Documento257 páginasInfertility 001Habtamu Nigussie100% (1)
- Reproductive Diseases (Male) : Disease Description Cause Cure / Remedy Picture Benign Prostatic Hypertrophy (BPH)Documento2 páginasReproductive Diseases (Male) : Disease Description Cause Cure / Remedy Picture Benign Prostatic Hypertrophy (BPH)sfsdfsdfAún no hay calificaciones
- Amenorrhea PDFDocumento5 páginasAmenorrhea PDFHeden ColladoAún no hay calificaciones
- CCD InfertilityDocumento26 páginasCCD InfertilityHanif GandohAún no hay calificaciones
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyDe EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyAún no hay calificaciones
- The Encyclopedia of Women's Health, Seventh EditionDe EverandThe Encyclopedia of Women's Health, Seventh EditionAún no hay calificaciones
- Pelvic Organ Prolapse: Prof Hossam HusseinDocumento71 páginasPelvic Organ Prolapse: Prof Hossam Husseinhossam626Aún no hay calificaciones
- Menopause and Voiding Troubles: Prof - Abdel Karim M. El HemalyDocumento29 páginasMenopause and Voiding Troubles: Prof - Abdel Karim M. El Hemalyhossam6260% (1)
- Obstetric Injuries To Genital Tract & Obstetric ShockDocumento34 páginasObstetric Injuries To Genital Tract & Obstetric Shockhossam626Aún no hay calificaciones
- إدارة الجودة الشاملة لضمان جودة الخدمات الصحية في المستشفيات - د. بن نافلة قدور، د. مزريق عاشورDocumento20 páginasإدارة الجودة الشاملة لضمان جودة الخدمات الصحية في المستشفيات - د. بن نافلة قدور، د. مزريق عاشورhossam626Aún no hay calificaciones
- The Cervix: Prof DR Hossam HusseinDocumento9 páginasThe Cervix: Prof DR Hossam Husseinhossam626Aún no hay calificaciones
- Hormone Replacement Therapy (HRT) Evidence-Based Guidelines: DR Mahdy El-Mazzahy Damietta General HospitalDocumento38 páginasHormone Replacement Therapy (HRT) Evidence-Based Guidelines: DR Mahdy El-Mazzahy Damietta General Hospitalhossam626Aún no hay calificaciones
- Ahmed Mohamed Abdel Rahim Rammah: Senior Registrar Obstetrics and Gynecology Department Al - Adan Hospital, KuwaitDocumento32 páginasAhmed Mohamed Abdel Rahim Rammah: Senior Registrar Obstetrics and Gynecology Department Al - Adan Hospital, Kuwaithossam626Aún no hay calificaciones
- Abnormal UterineDocumento23 páginasAbnormal Uterinehossam626Aún no hay calificaciones
- Review of Ovulation and Induction Protocolesal2Documento284 páginasReview of Ovulation and Induction Protocolesal2Hossamaldin Hussein Kamel SalemAún no hay calificaciones
- Physics of UltarasoundDocumento195 páginasPhysics of Ultarasoundhossam62683% (6)
- Contracted Pelvis: Cliquez Pour Modifier Le Style Des Sous-Titres Du MasqueDocumento10 páginasContracted Pelvis: Cliquez Pour Modifier Le Style Des Sous-Titres Du Masquehossam626Aún no hay calificaciones
- Non-Medelian Inheritance PDFDocumento12 páginasNon-Medelian Inheritance PDFbilly sauraAún no hay calificaciones
- Bu I 02 Time Allowed: 120 Minutes. Vocabulary - Grammar (4 PTS)Documento2 páginasBu I 02 Time Allowed: 120 Minutes. Vocabulary - Grammar (4 PTS)Linh BùiAún no hay calificaciones
- Antal Kizm (Geographical Feature)Documento21 páginasAntal Kizm (Geographical Feature)Cesar Man100% (1)
- Urea Plant Nangal 2014Documento8 páginasUrea Plant Nangal 2014Ishan HaiderAún no hay calificaciones
- Toxicology of Cleaning AgentsDocumento38 páginasToxicology of Cleaning AgentsThe AbyssinicansAún no hay calificaciones
- Medical and Psychiatric ComorbiditiesDocumento6 páginasMedical and Psychiatric ComorbiditiesDini indrianyAún no hay calificaciones
- Causes and Consequences of The American Civil WarDocumento5 páginasCauses and Consequences of The American Civil WarNhân PhanAún no hay calificaciones
- Nej M 200009073431001Documento8 páginasNej M 200009073431001Asri Ani NurchasanahAún no hay calificaciones
- Sterilization TechniquesDocumento6 páginasSterilization TechniquesKriyaAún no hay calificaciones
- Abstract Cagilkayan New1Documento2 páginasAbstract Cagilkayan New1cagilkayanAún no hay calificaciones
- Coconut Oil BenefitsDocumento2 páginasCoconut Oil BenefitsCharles Galan100% (1)
- VidyaDocumento15 páginasVidyadwitymoominAún no hay calificaciones
- Medical Surgical Nursing ReviewerDocumento8 páginasMedical Surgical Nursing ReviewerDavid Brillo0% (1)
- Smog Evs ProjectDocumento17 páginasSmog Evs Projectshrey narulaAún no hay calificaciones
- Dengue QayyumDocumento6 páginasDengue QayyumSyed Shahrul Naz SyedAún no hay calificaciones
- Mallappa Kumara Swamy - Plant-Derived Bioactives - Chemistry and Mode of Action-Springer Singapore - Springer (2020)Documento592 páginasMallappa Kumara Swamy - Plant-Derived Bioactives - Chemistry and Mode of Action-Springer Singapore - Springer (2020)Héctor Gómez YáñezAún no hay calificaciones
- At The Crossroads of Lipid Metabolism and InflammationDocumento7 páginasAt The Crossroads of Lipid Metabolism and InflammationChow Sing SingAún no hay calificaciones
- Excretion and HomeostasisDocumento6 páginasExcretion and HomeostasisVernonAún no hay calificaciones
- Diabetes Mellitus Surgical PatientDocumento33 páginasDiabetes Mellitus Surgical PatientGerald AndersonAún no hay calificaciones
- Antioxidant Effects of Astaxanthin in Various Diseases-A ReviewDocumento16 páginasAntioxidant Effects of Astaxanthin in Various Diseases-A ReviewHelenaAún no hay calificaciones
- Tuberculosis Prevention Plan: Histology LaboratoryDocumento10 páginasTuberculosis Prevention Plan: Histology LaboratoryLynel Joy JamotilloAún no hay calificaciones
- Other Health Impairment (OHI) : Teacher Tips/Learning StrategiesDocumento1 páginaOther Health Impairment (OHI) : Teacher Tips/Learning Strategiesapi-236207623Aún no hay calificaciones
- Chlamydia Power PointDocumento19 páginasChlamydia Power PointAnne McfarlandAún no hay calificaciones
- HQSS-ReportHigh-quality Health Systems in The Sustainable DevelopmentDocumento57 páginasHQSS-ReportHigh-quality Health Systems in The Sustainable DevelopmentDwi RahmawatiAún no hay calificaciones
- Reading Makkar - 1 - ! - at - #Documento155 páginasReading Makkar - 1 - ! - at - #dhrumil100% (6)
- Viro Final 6Documento10 páginasViro Final 6Muhammad Arslan UsmanAún no hay calificaciones
- Instant Download Solution Manual For Moneybanking and Financial Markets Cecchetti Schoenholtz 4th Edition PDF ScribdDocumento32 páginasInstant Download Solution Manual For Moneybanking and Financial Markets Cecchetti Schoenholtz 4th Edition PDF ScribdSharonYoungeizr100% (13)
- Oncology Nursing NotesDocumento12 páginasOncology Nursing Notesjoyrena ochondra100% (6)
- 11 - Manoj Kumar MinjDocumento8 páginas11 - Manoj Kumar MinjIndah SarihandayaniAún no hay calificaciones
- Secdocument - 61download Breast Pathology 2Nd Edition David J Dabbs Full ChapterDocumento67 páginasSecdocument - 61download Breast Pathology 2Nd Edition David J Dabbs Full Chapterjulia.swanson282100% (5)