También podría gustarte
- Polymyalgia Rheumatica, A Simple Guide To The Condition, Treatment And Related DiseasesDe EverandPolymyalgia Rheumatica, A Simple Guide To The Condition, Treatment And Related DiseasesCalificación: 5 de 5 estrellas5/5 (2)
- Faculty of MedicineDocumento28 páginasFaculty of MedicineRana AtefAún no hay calificaciones
- Arthritides 5th Year-UNZA LectureDocumento76 páginasArthritides 5th Year-UNZA LectureMohammed AadeelAún no hay calificaciones
- Musculoskeletal: Autoimmune Inflammatory Metabolic Infectious DisordersDocumento51 páginasMusculoskeletal: Autoimmune Inflammatory Metabolic Infectious DisordersSaya MenangAún no hay calificaciones
- Les Management - EditDocumento47 páginasLes Management - EditclaudiaciwiAún no hay calificaciones
- Myasthenia GravisDocumento4 páginasMyasthenia GravisArlyn MillanesAún no hay calificaciones
- Approach To Arthritis: Clinical GuideDocumento4 páginasApproach To Arthritis: Clinical GuideaveekumbharAún no hay calificaciones
- Mus1. Myasthenia GravisDocumento6 páginasMus1. Myasthenia GravisM AnnAún no hay calificaciones
- Motor Neurone Disease PDFDocumento4 páginasMotor Neurone Disease PDFTONY GO AWAYAún no hay calificaciones
- باطنة تمريض rheumatologyDocumento6 páginasباطنة تمريض rheumatologyAbdullmlik AlfurasAún no hay calificaciones
- Rhabdomyolysis: Pathogenesis, Diagnosis, and TreatmentDocumento12 páginasRhabdomyolysis: Pathogenesis, Diagnosis, and TreatmentSyifaAún no hay calificaciones
- Systemic LupusDocumento25 páginasSystemic LupusRana AtefAún no hay calificaciones
- Classification of Disorders of Musculoskeletal System (MSK) : Presented By: Siti Sarah Maha Dewi Bong Jen NeeDocumento69 páginasClassification of Disorders of Musculoskeletal System (MSK) : Presented By: Siti Sarah Maha Dewi Bong Jen NeeBONG AIKCHINGAún no hay calificaciones
- Been Hospitalized For 143 Days. ITP, TreatedDocumento78 páginasBeen Hospitalized For 143 Days. ITP, TreatedSutapa PawarAún no hay calificaciones
- Systemic Lupus Erythematosus Lecture Salah Abdel BakyDocumento8 páginasSystemic Lupus Erythematosus Lecture Salah Abdel Bakyahmed gabrAún no hay calificaciones
- 0009 Rheumatology Notes 2015 PDFDocumento56 páginas0009 Rheumatology Notes 2015 PDFMuhammad HaneefAún no hay calificaciones
- James Carter US Olympic Team Track & Field: Amitabh Bachchan Indian ActorDocumento22 páginasJames Carter US Olympic Team Track & Field: Amitabh Bachchan Indian ActorDummy AccountAún no hay calificaciones
- WEBINAR SLE HENDRATA (Final)Documento66 páginasWEBINAR SLE HENDRATA (Final)Wenny TanyawanAún no hay calificaciones
- Ankylosing SpondilitisDocumento38 páginasAnkylosing SpondilitisImelda JunaediAún no hay calificaciones
- ATAXIAS PTDocumento13 páginasATAXIAS PTKarunya VkAún no hay calificaciones
- Muscular Pathology: A. EpidemiologyDocumento4 páginasMuscular Pathology: A. EpidemiologyRitz CelsoAún no hay calificaciones
- Rheumatology MRCP1Documento186 páginasRheumatology MRCP1Raouf Ra'fat Soliman100% (3)
- Lupus Nephritis1Documento45 páginasLupus Nephritis1Lingga GumelarAún no hay calificaciones
- 2 RheumatologyDocumento31 páginas2 RheumatologySelim TarekAún no hay calificaciones
- Case Studies in Management of Muscle CrampsDocumento18 páginasCase Studies in Management of Muscle CrampsthiagoAún no hay calificaciones
- Identify The Etiology and Epidemiology ofDocumento3 páginasIdentify The Etiology and Epidemiology ofAllysahAún no hay calificaciones
- Autoimmune DisordersDocumento88 páginasAutoimmune DisordersJR Rolf NeuqeletAún no hay calificaciones
- Core Knowledge For Pro Exam-1Documento4 páginasCore Knowledge For Pro Exam-1Shaheera ShamsudinAún no hay calificaciones
- Systemic Inflammatory Response Syndrome (SIRS) : Pranee Sitaposa, MDDocumento43 páginasSystemic Inflammatory Response Syndrome (SIRS) : Pranee Sitaposa, MDAli TawbeAún no hay calificaciones
- PasquiniM2 DM AID07vzsaDocumento12 páginasPasquiniM2 DM AID07vzsaYeni Chie Aneuk TuleutAún no hay calificaciones
- Amyotrophic Lateral SclerosisDocumento9 páginasAmyotrophic Lateral SclerosisCaroline ItnerAún no hay calificaciones
- Neurology, NeuromuscularDisorders-MRyanDocumento82 páginasNeurology, NeuromuscularDisorders-MRyanFiras SawanAún no hay calificaciones
- B. Immunosuppressive Therapy: Video 11Documento9 páginasB. Immunosuppressive Therapy: Video 11Bianx Flores DosdosAún no hay calificaciones
- Acute Lymphoblastic Leukemia DR - Hussein AlatabiDocumento21 páginasAcute Lymphoblastic Leukemia DR - Hussein AlatabiSaman SarKoAún no hay calificaciones
- SpondylitisDocumento28 páginasSpondylitisjesmitha2740Aún no hay calificaciones
- Spektrum AIDocumento55 páginasSpektrum AIOgizWaraAún no hay calificaciones
- Enfermedades LisosomalesDocumento32 páginasEnfermedades LisosomalesJonathanOmarLaraAcevedoAún no hay calificaciones
- Myasthenia Gravis and Other Neuromuscular Junction DisordersDocumento8 páginasMyasthenia Gravis and Other Neuromuscular Junction Disordersidno1008Aún no hay calificaciones
- Renal Transplant CaseDocumento3 páginasRenal Transplant CaseSantosh ParabAún no hay calificaciones
- Rheumatoid ArthritisDocumento6 páginasRheumatoid ArthritishoneyAún no hay calificaciones
- Ziad Aro, MD Internal MedicineDocumento91 páginasZiad Aro, MD Internal MedicineAli Aborges Jr.Aún no hay calificaciones
- Vasculitis: VASCULITIS Is A Primary Inflammatory Disease Process of The VasculatureDocumento43 páginasVasculitis: VASCULITIS Is A Primary Inflammatory Disease Process of The VasculaturelihayatiAún no hay calificaciones
- Morning Report: Aaron Mccoy, MD, Pgy3Documento16 páginasMorning Report: Aaron Mccoy, MD, Pgy3Emily EresumaAún no hay calificaciones
- Musculoskeletal: Autoimmune Inflammatory Metabolic Infectious DisordersDocumento51 páginasMusculoskeletal: Autoimmune Inflammatory Metabolic Infectious DisordersHarshoi KrishannaAún no hay calificaciones
- Spondyloarthritis ResidentDocumento70 páginasSpondyloarthritis Residentviraaj pawar100% (1)
- Multiple MyelomaDocumento34 páginasMultiple Myelomad clarkeAún no hay calificaciones
- James Carter US Olympic Team Track & Field: Amitabh Bachchan Indian ActorDocumento22 páginasJames Carter US Olympic Team Track & Field: Amitabh Bachchan Indian ActorSri KombongAún no hay calificaciones
- Systemic Lupus Erythematosus, Rheumatoid ArthritisDocumento28 páginasSystemic Lupus Erythematosus, Rheumatoid ArthritisSalomeSibashviliAún no hay calificaciones
- Donna-Marie Mcmahon, Do, Faap Kathleen M. Vazzana, Do, MsDocumento13 páginasDonna-Marie Mcmahon, Do, Faap Kathleen M. Vazzana, Do, MsMuhammad GassanAún no hay calificaciones
- Arthritis 180325095830 PDFDocumento77 páginasArthritis 180325095830 PDFHesoca HuxAún no hay calificaciones
- Screenshot 2022-02-04 at 8.43.02 PMDocumento23 páginasScreenshot 2022-02-04 at 8.43.02 PMAws MahmoudAún no hay calificaciones
- Transverse Myelitis: Differential DiagnosisDocumento14 páginasTransverse Myelitis: Differential DiagnosissekiannAún no hay calificaciones
- Concept Map Aplastic Anemia 212 1Documento1 páginaConcept Map Aplastic Anemia 212 1S AustinAún no hay calificaciones
- Panduan Praktik Klinik (PPK) Departemen/Smf Penyakit Dalam Rsud KH Daud Arif Lupus Eritematosus Sistemik (Les) Kode: ICD. 10. M32Documento33 páginasPanduan Praktik Klinik (PPK) Departemen/Smf Penyakit Dalam Rsud KH Daud Arif Lupus Eritematosus Sistemik (Les) Kode: ICD. 10. M32Anonymous aBbQD8oyjJAún no hay calificaciones
- Ankylosing Spondylitis: Submitted by Safeer Mohammed S 302 General Medicine Submitted To Dr. Marietta DavidianDocumento20 páginasAnkylosing Spondylitis: Submitted by Safeer Mohammed S 302 General Medicine Submitted To Dr. Marietta DavidianSafeer VarkalaAún no hay calificaciones
- Rheuma 2018Documento111 páginasRheuma 2018abdulahad mohamedAún no hay calificaciones
- CV Complication SCIDocumento28 páginasCV Complication SCIcris weeAún no hay calificaciones
- Traditional Treatments Vs Moder Treatments For ALSDocumento63 páginasTraditional Treatments Vs Moder Treatments For ALSSnezana MihajlovicAún no hay calificaciones
- Logy - Toronto NotesDocumento36 páginasLogy - Toronto NotesAndré de QueirozAún no hay calificaciones
- Medicine Exam NotesDocumento211 páginasMedicine Exam Notesjf65ky8f8tAún no hay calificaciones
- Anti-Inflammatory Drugs Даша ОкончательнDocumento82 páginasAnti-Inflammatory Drugs Даша ОкончательнHerry HendrayadiAún no hay calificaciones
- The Top 10 Generic Pharmaceutical CompaniesDocumento10 páginasThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiAún no hay calificaciones
- BCP 13010 PDFDocumento11 páginasBCP 13010 PDFHerry HendrayadiAún no hay calificaciones
- Astellas Pharma: Launches Irribow OD Tablets in Japan For Diarrhea-Predominant Irritable Bowel SyndromeDocumento3 páginasAstellas Pharma: Launches Irribow OD Tablets in Japan For Diarrhea-Predominant Irritable Bowel SyndromeHerry HendrayadiAún no hay calificaciones
- 1 - Dr. KungDocumento18 páginas1 - Dr. KungWawan IndrawanAún no hay calificaciones
- The Top 10 Generic Pharmaceutical CompaniesDocumento42 páginasThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiAún no hay calificaciones
- Practical Guide To Joint and Soft Tissue Injection TechniquesDocumento5 páginasPractical Guide To Joint and Soft Tissue Injection TechniquesHerry HendrayadiAún no hay calificaciones
- Press Conference: Astellas' Growth StrategyDocumento31 páginasPress Conference: Astellas' Growth StrategyHerry HendrayadiAún no hay calificaciones
- Standard Step-Wise Timelines in The Drug Discovery ProcessDocumento19 páginasStandard Step-Wise Timelines in The Drug Discovery ProcessHerry HendrayadiAún no hay calificaciones
- Growth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsDocumento176 páginasGrowth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsHerry HendrayadiAún no hay calificaciones
- Lifecycle Management Strategies Maximizing ROI Through Indication Expansion Reformulation and Rx-To-OTC SwitchingDocumento176 páginasLifecycle Management Strategies Maximizing ROI Through Indication Expansion Reformulation and Rx-To-OTC SwitchingHerry Hendrayadi100% (1)
- The Global AntiInfectives Market OutlookDocumento267 páginasThe Global AntiInfectives Market OutlookHerry HendrayadiAún no hay calificaciones
- The Global AntiInfectives Market OutlookDocumento267 páginasThe Global AntiInfectives Market OutlookHerry HendrayadiAún no hay calificaciones
- Standard Step-Wise Timelines in The Drug Discovery ProcessDocumento19 páginasStandard Step-Wise Timelines in The Drug Discovery ProcessHerry HendrayadiAún no hay calificaciones
- Global Market AnalysisaAntibioticsDocumento23 páginasGlobal Market AnalysisaAntibioticsHerry HendrayadiAún no hay calificaciones
- Indication Expansion Opportunities For Successful Lifecycle ManagementDocumento144 páginasIndication Expansion Opportunities For Successful Lifecycle ManagementHerry HendrayadiAún no hay calificaciones
- Pharmaceutical Growth Opportunities in Brazil, Russia, India and ChinaDocumento35 páginasPharmaceutical Growth Opportunities in Brazil, Russia, India and ChinaHerry HendrayadiAún no hay calificaciones
- The Top 10 Generic Pharmaceutical CompaniesDocumento42 páginasThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiAún no hay calificaciones
- Top 10 Generic Pharmaceutical CompaniesDocumento178 páginasTop 10 Generic Pharmaceutical CompaniesHerry HendrayadiAún no hay calificaciones
- The Blockbuster Drugs Outlook PDFDocumento259 páginasThe Blockbuster Drugs Outlook PDFHerry HendrayadiAún no hay calificaciones
- Top 15 Therapeutic 2008 PDFDocumento95 páginasTop 15 Therapeutic 2008 PDFHerry HendrayadiAún no hay calificaciones
- Achieving Market Dominance Through Reformulation.Documento12 páginasAchieving Market Dominance Through Reformulation.Herry HendrayadiAún no hay calificaciones
- Achieving Market Dominance Through ReformulationDocumento223 páginasAchieving Market Dominance Through ReformulationHerry HendrayadiAún no hay calificaciones
- Management Pocketbooks - The Balance Sheet PocketbookDocumento309 páginasManagement Pocketbooks - The Balance Sheet PocketbookHerry Hendrayadi100% (1)
- 2nd Announcement A5 Upload 1Documento18 páginas2nd Announcement A5 Upload 1Herry HendrayadiAún no hay calificaciones
- Growth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsDocumento176 páginasGrowth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsHerry HendrayadiAún no hay calificaciones
- Reader's Digest January 2013Documento148 páginasReader's Digest January 2013pereira_jus3430Aún no hay calificaciones
- Pharma 2020 PWC ReportDocumento32 páginasPharma 2020 PWC ReportBrand SynapseAún no hay calificaciones
- Ijss Aug Oa12Documento5 páginasIjss Aug Oa12Herry HendrayadiAún no hay calificaciones
- Systemic Lupus Erythematosus and Neuropsychiatric DiseaseDocumento56 páginasSystemic Lupus Erythematosus and Neuropsychiatric DiseaseHerry HendrayadiAún no hay calificaciones
- Synthesis PaperDocumento6 páginasSynthesis Paperapi-252076032Aún no hay calificaciones
- Antistreptolysin - O (ASO) Latex TestDocumento2 páginasAntistreptolysin - O (ASO) Latex Testalejandra niñoAún no hay calificaciones
- Immunology & Immunotechnology - 1Documento40 páginasImmunology & Immunotechnology - 1jihovajayraAún no hay calificaciones
- SYPHILIS in Pregnancy CDCDocumento5 páginasSYPHILIS in Pregnancy CDCDiana NeculceaAún no hay calificaciones
- The Bubonic Plague, Spanish Flu and Covid 19Documento16 páginasThe Bubonic Plague, Spanish Flu and Covid 19maia harnauthAún no hay calificaciones
- Goat Cheesy GlandDocumento3 páginasGoat Cheesy GlandSidonSaagarVincentAún no hay calificaciones
- Control of Diarrheal DiseasesDocumento57 páginasControl of Diarrheal Diseaseshjl padillaAún no hay calificaciones
- Basics of HIVDocumento32 páginasBasics of HIVAudry NurulAún no hay calificaciones
- Staphylococcus Aureus: Ali Somily MD, FRCPCDocumento32 páginasStaphylococcus Aureus: Ali Somily MD, FRCPCraanja2Aún no hay calificaciones
- Recurrent Mycobacterium Tuberculosis Infection in Systemic Lupus Erythematosus Patient Case Report and ReviewDocumento8 páginasRecurrent Mycobacterium Tuberculosis Infection in Systemic Lupus Erythematosus Patient Case Report and ReviewpaulallenfileAún no hay calificaciones
- Guide To Biologic Therapy 1Documento24 páginasGuide To Biologic Therapy 1Andra GarbeaAún no hay calificaciones
- 4life Transfer Factor: Which Product Is Right For Me?Documento1 página4life Transfer Factor: Which Product Is Right For Me?jhimsyAún no hay calificaciones
- Immuno FluorescenceDocumento2 páginasImmuno FluorescenceEstiak RonyAún no hay calificaciones
- Skin Prick TestDocumento3 páginasSkin Prick TestRiyanda FurqanAún no hay calificaciones
- CertificateDocumento1 páginaCertificateRanjana RanjanaAún no hay calificaciones
- Prof. Beata Sobieszczańska Wrocław Medical University Dept. of MicrobiologyDocumento44 páginasProf. Beata Sobieszczańska Wrocław Medical University Dept. of MicrobiologyBeata SobieszczańskaAún no hay calificaciones
- Dengue Final Case Report Ready - OdtDocumento5 páginasDengue Final Case Report Ready - Odtroshan bhandariAún no hay calificaciones
- CBC InterpretationDocumento6 páginasCBC InterpretationKate Basa100% (1)
- Passive Voice PDFDocumento2 páginasPassive Voice PDFalya nafaAún no hay calificaciones
- Module 6 Student Activity SheetDocumento7 páginasModule 6 Student Activity SheetJenny Agustin FabrosAún no hay calificaciones
- Reading Practice - ChickenpoxDocumento4 páginasReading Practice - ChickenpoxDavid Jr.Aún no hay calificaciones
- 202110 강의자료Documento107 páginas202110 강의자료kim hwiAún no hay calificaciones
- Parasitology Micro D&R AgamDocumento108 páginasParasitology Micro D&R AgamNirosha Arul100% (1)
- Metastatic Infection During Staphylococcus Aureus Bacteremia 2020 PDFDocumento8 páginasMetastatic Infection During Staphylococcus Aureus Bacteremia 2020 PDFJ Sebastian PeinadoAún no hay calificaciones
- Sonu Kumar Yadav COVID ReportDocumento1 páginaSonu Kumar Yadav COVID ReportVeeraj SinghAún no hay calificaciones
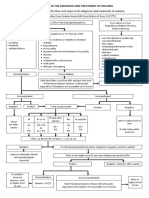
- Algorithm in The Diagnosis and Treatment of MalariaDocumento1 páginaAlgorithm in The Diagnosis and Treatment of MalariaPearl Monette Cedeño AngAún no hay calificaciones
- Archer (Staphylococcus Aureus)Documento3 páginasArcher (Staphylococcus Aureus)_meiantiAún no hay calificaciones
- Influenza 1Documento5 páginasInfluenza 1Angeli Jean Koreen CorpuzAún no hay calificaciones
- The Immune Effects of An African Traditional EnergDocumento14 páginasThe Immune Effects of An African Traditional Energthan vergaraAún no hay calificaciones
- Head Neck Infections Obstructive Airway Disease FactsDocumento17 páginasHead Neck Infections Obstructive Airway Disease FactscrystalsheAún no hay calificaciones