También podría gustarte
- Problem-based Approach to Gastroenterology and HepatologyDe EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisAún no hay calificaciones
- Reye SyndromeDocumento10 páginasReye SyndromeDanil KhairulAún no hay calificaciones
- Renal Tubular AcidosisDocumento48 páginasRenal Tubular Acidosissny PAún no hay calificaciones
- SIADH, DI, Cerebral Salt WastingDocumento20 páginasSIADH, DI, Cerebral Salt Wastingmaged_najehAún no hay calificaciones
- SAMDocumento108 páginasSAMAlimyon Abilar MontoloAún no hay calificaciones
- National Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaDocumento53 páginasNational Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaNational Dengue Control Unit,Sri Lanka100% (1)
- ThalassemiaDocumento16 páginasThalassemiaAry AffandiAún no hay calificaciones
- TORCH InfectionsDocumento37 páginasTORCH InfectionsEylin Halim Rahardjo100% (1)
- Cerebrovascular Disease (Bleed)Documento25 páginasCerebrovascular Disease (Bleed)Margaret Jenaw JenawAún no hay calificaciones
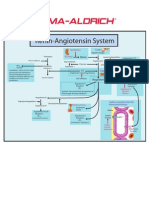
- Renin-Angiotensin SystemDocumento1 páginaRenin-Angiotensin SystemSigma-Aldrich100% (2)
- VOD - SOS in HSCTDocumento25 páginasVOD - SOS in HSCTKim-Thinh Nguyen ThiAún no hay calificaciones
- ThalassemiaDocumento24 páginasThalassemiaapi-459076195Aún no hay calificaciones
- Neonatal Jaundice Clinical Presentation - History, Physical Examination PDFDocumento5 páginasNeonatal Jaundice Clinical Presentation - History, Physical Examination PDFPaola Méndez NeciosupAún no hay calificaciones
- Acute Rheumatic Heart DiseaseDocumento25 páginasAcute Rheumatic Heart DiseaseArun GeorgeAún no hay calificaciones
- History: Symptoms Associated With Specific Viral InfectionsDocumento12 páginasHistory: Symptoms Associated With Specific Viral InfectionsFatima Love Ariate-ArcasetasAún no hay calificaciones
- ALL Pulmonary Leukostasis2Documento6 páginasALL Pulmonary Leukostasis2Pratita Jati PermatasariAún no hay calificaciones
- Type B (Hib) Vaccine: Haemophilus InfluenzaeDocumento2 páginasType B (Hib) Vaccine: Haemophilus InfluenzaeEnce MalatambanAún no hay calificaciones
- Case Study 2Documento4 páginasCase Study 2api-2451636590% (1)
- Essensial Hypertension Pathogenesis and PathophsiologyDocumento22 páginasEssensial Hypertension Pathogenesis and PathophsiologyAmeliana KamaludinAún no hay calificaciones
- Hodgkin's DiseaseDocumento58 páginasHodgkin's Diseasealibayaty1Aún no hay calificaciones
- Clinical Features of Renal DiseaseDocumento80 páginasClinical Features of Renal DiseaseIdiAmadouAún no hay calificaciones
- A Case Study of Epidural HematomaDocumento27 páginasA Case Study of Epidural HematomaNeil GoAún no hay calificaciones
- Case Protocol Kawasaki DiseaseDocumento5 páginasCase Protocol Kawasaki DiseaseFranz SalazarAún no hay calificaciones
- Pediatric Assesment Tool: Sakit Jud Siya, Mga 8 Siguro."Documento5 páginasPediatric Assesment Tool: Sakit Jud Siya, Mga 8 Siguro."RubelleMicahCagampangSapongAún no hay calificaciones
- Pediatric Imperforate Anus - Background, Pathophysiology, EpidemiologyDocumento4 páginasPediatric Imperforate Anus - Background, Pathophysiology, EpidemiologyYehuda Agus SantosoAún no hay calificaciones
- DR Amanullah Lail: Assistant Professor Paediatrics Duhs/Dmc/ChkDocumento36 páginasDR Amanullah Lail: Assistant Professor Paediatrics Duhs/Dmc/ChkpaqardAún no hay calificaciones
- PSGNDocumento23 páginasPSGNalpha mae beltranAún no hay calificaciones
- Cyclic VomitingDocumento19 páginasCyclic VomitingEmily EresumaAún no hay calificaciones
- Pat 2 Medsurg1Documento20 páginasPat 2 Medsurg1api-300849832Aún no hay calificaciones
- Renal Concept MapDocumento8 páginasRenal Concept MapXtine CajiAún no hay calificaciones
- Case Presentation-ChickenpoxDocumento41 páginasCase Presentation-ChickenpoxShaliniAún no hay calificaciones
- HepatosplenomegalyDocumento49 páginasHepatosplenomegalyTarun SinghAún no hay calificaciones
- Acute Rheumatic FeverDocumento5 páginasAcute Rheumatic FeverSyahmi AhmadAún no hay calificaciones
- Spontaneous Bacterial Peritonitis (SBP) & AsciticDocumento15 páginasSpontaneous Bacterial Peritonitis (SBP) & AsciticFebi RahmadinAún no hay calificaciones
- EclampsiaDocumento56 páginasEclampsiagalihtrimuninggarAún no hay calificaciones
- Cardiomyopathy: Imtiyaz Ali Lecturer, UTARDocumento31 páginasCardiomyopathy: Imtiyaz Ali Lecturer, UTARSalman KhanAún no hay calificaciones
- DIC Case StudyDocumento7 páginasDIC Case StudyRobertAún no hay calificaciones
- Blood Transfusions PPT Presentation - Rachelle ArcuriDocumento14 páginasBlood Transfusions PPT Presentation - Rachelle Arcuriapi-242208706Aún no hay calificaciones
- Diabetes MellitusDocumento17 páginasDiabetes MellitusRuqayya KobatteAún no hay calificaciones
- Anak 3.1 Infective Endocarditis DRTLTDocumento21 páginasAnak 3.1 Infective Endocarditis DRTLTAnastasia PinkyAún no hay calificaciones
- Hiv in Pregnancy FinalDocumento73 páginasHiv in Pregnancy Finalapi-3797079Aún no hay calificaciones
- Hiv Case StudyDocumento2 páginasHiv Case Studyapi-485814878Aún no hay calificaciones
- CBC InterpretationDocumento6 páginasCBC InterpretationKate Basa100% (1)
- Pathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionDocumento2 páginasPathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionMauliza Resky NisaAún no hay calificaciones
- Exchange Blood TransfusionDocumento38 páginasExchange Blood TransfusionMeseret Hamer Zewdie100% (1)
- Psychological Task of Pregnancy Danger Signs of Pregnancy: 4. Past Medical HistoryDocumento6 páginasPsychological Task of Pregnancy Danger Signs of Pregnancy: 4. Past Medical HistoryKimberly Sharah Mae Fortuno100% (1)
- Pediatric Community-Acquired Pneumonia Clinical Guideline PDFDocumento1 páginaPediatric Community-Acquired Pneumonia Clinical Guideline PDFJohn Vincent Dy OcampoAún no hay calificaciones
- Sheehan SyndromeDocumento6 páginasSheehan SyndromeArvie TagnongAún no hay calificaciones
- Congenital SyphilisDocumento6 páginasCongenital SyphilisFrozen Pandora MahayaAún no hay calificaciones
- Tetralogy of Fallot (TF)Documento25 páginasTetralogy of Fallot (TF)Safira RAún no hay calificaciones
- Enuresis in Children - A Case - Based ApproachDocumento9 páginasEnuresis in Children - A Case - Based ApproachBogdan NeamtuAún no hay calificaciones
- Meconium AspirationDocumento23 páginasMeconium AspirationWitneyGraceAún no hay calificaciones
- Bronchiolitis Clinical Practice GuidelineDocumento21 páginasBronchiolitis Clinical Practice GuidelineJuwita PratiwiAún no hay calificaciones
- History and Physical Examination in Pediatrics (1) - 1Documento44 páginasHistory and Physical Examination in Pediatrics (1) - 1okwadha simion100% (1)
- Acute Glomerulonephritis: Group 8 PresentationDocumento25 páginasAcute Glomerulonephritis: Group 8 PresentationcollinsmagAún no hay calificaciones
- Cyclic Vomiting SyndromeDocumento17 páginasCyclic Vomiting Syndromeminerva_stanciuAún no hay calificaciones
- Cardiac Conditions Cardiac Dysrhythmias: B. Sinus BradycardiaDocumento5 páginasCardiac Conditions Cardiac Dysrhythmias: B. Sinus BradycardiaIrish Eunice FelixAún no hay calificaciones
- Management of Tuberculosis: A guide for clinicians (eBook edition)De EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Aún no hay calificaciones
- Asthma in Children: Chronic Asthma & Achieving ControlDocumento75 páginasAsthma in Children: Chronic Asthma & Achieving ControlNyomanGinaHennyKristiantiAún no hay calificaciones
- A Randomized Controlled Trial Comparing The Effect of Fortification of Human Milk With An Infant Formula Powder Versus Unfortified Human Milk On TheDocumento3 páginasA Randomized Controlled Trial Comparing The Effect of Fortification of Human Milk With An Infant Formula Powder Versus Unfortified Human Milk On TheNyomanGinaHennyKristiantiAún no hay calificaciones
- Cat Tembok Tinting Lenkote Aquamatt Interior 25 KG Paket Google ShoppingDocumento1 páginaCat Tembok Tinting Lenkote Aquamatt Interior 25 KG Paket Google ShoppingNyomanGinaHennyKristiantiAún no hay calificaciones
- Nop Rev - 19Documento8 páginasNop Rev - 19NyomanGinaHennyKristiantiAún no hay calificaciones
- JurnalDocumento10 páginasJurnalNyomanGinaHennyKristiantiAún no hay calificaciones
- Leptin Insulin and Thyroid Hormones in A Cohort ofDocumento8 páginasLeptin Insulin and Thyroid Hormones in A Cohort ofNyomanGinaHennyKristiantiAún no hay calificaciones
- Urine Electrolytes PDFDocumento26 páginasUrine Electrolytes PDFNyomanGinaHennyKristiantiAún no hay calificaciones
- Compensated Dengue Shock Syndrome (A97.2) and Obesity (E.661)Documento3 páginasCompensated Dengue Shock Syndrome (A97.2) and Obesity (E.661)NyomanGinaHennyKristiantiAún no hay calificaciones
- Daftar PustakaDocumento1 páginaDaftar PustakaNyomanGinaHennyKristiantiAún no hay calificaciones
- JadwalDocumento5 páginasJadwalNyomanGinaHennyKristiantiAún no hay calificaciones
- 873 FullDocumento5 páginas873 FullNyomanGinaHennyKristiantiAún no hay calificaciones
- GI Problems in Early Life EditDocumento59 páginasGI Problems in Early Life EditNyomanGinaHennyKristiantiAún no hay calificaciones
- Brain AbscessDocumento10 páginasBrain AbscesstrujilloAún no hay calificaciones
- Trace Element EpilepsyDocumento8 páginasTrace Element EpilepsyNyomanGinaHennyKristiantiAún no hay calificaciones
- Lyophilised Saccharomyces Boulardii: Contoh ProbiotikDocumento1 páginaLyophilised Saccharomyces Boulardii: Contoh ProbiotikNyomanGinaHennyKristiantiAún no hay calificaciones
- Sticker NameDocumento2 páginasSticker NameNyomanGinaHennyKristiantiAún no hay calificaciones
- Cover GastroDocumento1 páginaCover GastroNyomanGinaHennyKristiantiAún no hay calificaciones
- A Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)Documento7 páginasA Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)NyomanGinaHennyKristiantiAún no hay calificaciones
- Surgery FinalDocumento102 páginasSurgery FinalfilchibuffAún no hay calificaciones
- Daftar Pustaka: Dalam, Edisi 1, Balai Penerbit FKUI, JakartaDocumento2 páginasDaftar Pustaka: Dalam, Edisi 1, Balai Penerbit FKUI, JakartaNyomanGinaHennyKristiantiAún no hay calificaciones
- Daftar Pustaka: Eur J PediatrDocumento4 páginasDaftar Pustaka: Eur J PediatrNyomanGinaHennyKristiantiAún no hay calificaciones
- Commissioning Valve Product BrochureDocumento14 páginasCommissioning Valve Product BrochureblindjaxxAún no hay calificaciones
- Product Analysis Certificate: Propanol-2 (Iso-Propanol) A.RDocumento1 páginaProduct Analysis Certificate: Propanol-2 (Iso-Propanol) A.RAMMARAún no hay calificaciones
- Honda Bikes and ScootersDocumento6 páginasHonda Bikes and ScootersShamrjit AgrahariAún no hay calificaciones
- Functional Endoscopic Sinus SurgeryDocumento3 páginasFunctional Endoscopic Sinus SurgeryDanielicah CruzAún no hay calificaciones
- Perbedaan Fermentasi Dan Respirasi Anaerob (Campbell Biology 12th Ed.)Documento4 páginasPerbedaan Fermentasi Dan Respirasi Anaerob (Campbell Biology 12th Ed.)Oppof7 OppoAún no hay calificaciones
- Method Statement For Boom Barrier Installation (Rev00) ELV2Documento38 páginasMethod Statement For Boom Barrier Installation (Rev00) ELV2balajiAún no hay calificaciones
- MIMSDocumento3 páginasMIMSFrancineAntoinetteGonzalesAún no hay calificaciones
- Dimensional Stability After MoldingDocumento14 páginasDimensional Stability After MoldingpgovindaiahAún no hay calificaciones
- 12abmb2 Group4 Chapter1Documento20 páginas12abmb2 Group4 Chapter1Kenneth Del RosarioAún no hay calificaciones
- Rama Varma Anagha Research PaperDocumento12 páginasRama Varma Anagha Research Paperapi-308560676Aún no hay calificaciones
- Bravo Petroleum ProfileDocumento8 páginasBravo Petroleum ProfileJacob Thom ZiwahwaAún no hay calificaciones
- English: Third Quarter - Module 3Documento12 páginasEnglish: Third Quarter - Module 3Anna Agravante-SulitAún no hay calificaciones
- System Substation Commissioning TestsDocumento8 páginasSystem Substation Commissioning TestsCvijayakumar100% (1)
- Gujarat-Ports Sector ReportDocumento17 páginasGujarat-Ports Sector ReportK. Ashok Vardhan ShettyAún no hay calificaciones
- 5980 10143 1 SM PDFDocumento11 páginas5980 10143 1 SM PDFfaustinaAún no hay calificaciones
- Neurology Condition Assessment Methods: Guillain-Barre Syndrome (GBS) Disability ScoreDocumento15 páginasNeurology Condition Assessment Methods: Guillain-Barre Syndrome (GBS) Disability ScoreMrinmayeeDeshmukhAún no hay calificaciones
- LLM01v5 0Documento12 páginasLLM01v5 0Alan LeungAún no hay calificaciones
- Lista de Productos Nov 2018Documento10 páginasLista de Productos Nov 2018MoisesManuelBravoLeonAún no hay calificaciones
- Serial Interface RS485 (RS422) Configuration InstructionsDocumento20 páginasSerial Interface RS485 (RS422) Configuration Instructionsyana sopian hidayatAún no hay calificaciones
- Wahabism - Bala SurajoDocumento17 páginasWahabism - Bala SurajoAbu Muhammad50% (2)
- Tuesday 12 January 2021: ChemistryDocumento24 páginasTuesday 12 January 2021: Chemistryuchi haAún no hay calificaciones
- Subcontracting Process in Production - SAP BlogsDocumento12 páginasSubcontracting Process in Production - SAP Blogsprasanna0788Aún no hay calificaciones
- Design & Fabrication of Low Cost Small-Scale Fatigue Testing MachineDocumento12 páginasDesign & Fabrication of Low Cost Small-Scale Fatigue Testing MachinekshitijAún no hay calificaciones
- Allegheny Power Planning CriteriaDocumento19 páginasAllegheny Power Planning Criteriaksdp1Aún no hay calificaciones
- MEC Threads ChartDocumento12 páginasMEC Threads ChartenricoAún no hay calificaciones
- RAJPUT - Gokul IndustryDocumento76 páginasRAJPUT - Gokul IndustryrajputvjAún no hay calificaciones
- Biology: Higher Tier Paper 1HDocumento28 páginasBiology: Higher Tier Paper 1HkaruneshnAún no hay calificaciones
- GENII - Nissan Patrol GQ & GU - RE4 4 Speed Diesel & Petrol - Lock Up Instructions-1Documento14 páginasGENII - Nissan Patrol GQ & GU - RE4 4 Speed Diesel & Petrol - Lock Up Instructions-1Trav GilesAún no hay calificaciones
- Safe and Gentle Ventilation For Little Patients Easy - Light - SmartDocumento4 páginasSafe and Gentle Ventilation For Little Patients Easy - Light - SmartSteven BrownAún no hay calificaciones