También podría gustarte
- An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentDe EverandAn Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentBaharudin AbdullahAún no hay calificaciones
- SurgeryDocumento135 páginasSurgeryAndi AlfianAún no hay calificaciones
- Ca PenisDocumento25 páginasCa Penisrajan kumar100% (2)
- DSTC 0309-Dcs & DCR UpdatedDocumento124 páginasDSTC 0309-Dcs & DCR UpdatedDenny TombengAún no hay calificaciones
- Injuries To Genito-Urinary Tract: Dr. Ramlan Nasution, Sp.U / Dr. Yacobda H. Sigumonrong, Sp.UDocumento63 páginasInjuries To Genito-Urinary Tract: Dr. Ramlan Nasution, Sp.U / Dr. Yacobda H. Sigumonrong, Sp.UAulia SiregarAún no hay calificaciones
- ATLS Initial Assessment and ManagementDocumento21 páginasATLS Initial Assessment and Managementazisfitri100% (2)
- ATLS Chapter Spine and Spinal Cord InjuryDocumento29 páginasATLS Chapter Spine and Spinal Cord InjuryFahmi AnshoriAún no hay calificaciones
- Matary Differential Diagnosis 2013 PDFDocumento128 páginasMatary Differential Diagnosis 2013 PDFAlejandra Rozo BayerAún no hay calificaciones
- Vascular Diseases: Idar Mappangara Department of Cardiology Hasanuddin UniversityDocumento31 páginasVascular Diseases: Idar Mappangara Department of Cardiology Hasanuddin UniversityHariadhii SalamAún no hay calificaciones
- Pancoast TumorDocumento26 páginasPancoast TumorDhanis HastinAún no hay calificaciones
- Growth Plate InjuriesDocumento41 páginasGrowth Plate Injurieskosmynin86Aún no hay calificaciones
- Pediatric: Abdulrahman Y. SabbaghDocumento36 páginasPediatric: Abdulrahman Y. SabbaghAbdulrahman Y. SabbaghAún no hay calificaciones
- Angle Closure GlaucomaDocumento6 páginasAngle Closure GlaucomaRick van DewAún no hay calificaciones
- Department of Surgery Songkhla HospitalDocumento31 páginasDepartment of Surgery Songkhla HospitalFerdinand AllotodangAún no hay calificaciones
- Closed Head Injury CPG 2nd Ed Algorithm 2Documento1 páginaClosed Head Injury CPG 2nd Ed Algorithm 2Nick PaulAún no hay calificaciones
- Basal Cell Carcinoma of The Eye Lid by Thea Umbac, Ophthalmology InternDocumento32 páginasBasal Cell Carcinoma of The Eye Lid by Thea Umbac, Ophthalmology InternThea SelinaAún no hay calificaciones
- Spleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementDocumento53 páginasSpleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementMuhammad SaadAún no hay calificaciones
- Endoscopic Third Ventriculostomy For The Management of ChiariDocumento34 páginasEndoscopic Third Ventriculostomy For The Management of ChiariYagatheeswaran KetheeswaranAún no hay calificaciones
- Neet StuffDocumento26 páginasNeet StuffBalasubrahmanya K. R.Aún no hay calificaciones
- CraniosynostosisDocumento12 páginasCraniosynostosisWaeel HamoudaAún no hay calificaciones
- Hepatobiliary Notes 2.0Documento18 páginasHepatobiliary Notes 2.0Sri VathanahAún no hay calificaciones
- Station 5 CluesDocumento41 páginasStation 5 CluesSagit Nauman81Aún no hay calificaciones
- Slide Fraktur FemurDocumento26 páginasSlide Fraktur FemurMarhama FitrianiAún no hay calificaciones
- BoneDocumento68 páginasBonedr_asaleh100% (2)
- Ocular Emergencies TraumaDocumento35 páginasOcular Emergencies TraumaMochaLover100% (2)
- Spindle Cell TumorsDocumento138 páginasSpindle Cell TumorsMadhura ShekatkarAún no hay calificaciones
- 8 4 13notesDocumento437 páginas8 4 13notesJesse GriffithAún no hay calificaciones
- Neuroradiology: Sony Sutrisno Department of Radiology Krida Wacana Christian UniversityDocumento46 páginasNeuroradiology: Sony Sutrisno Department of Radiology Krida Wacana Christian UniversityPaulus AnungAún no hay calificaciones
- Melanoma: Meku Damtie (M.D.) July 18, 2006Documento38 páginasMelanoma: Meku Damtie (M.D.) July 18, 2006Worku KifleAún no hay calificaciones
- Surgery ParathyroidDocumento11 páginasSurgery ParathyroidMATTHEW EARL MALUMAYAún no hay calificaciones
- Chest Trauma3Documento120 páginasChest Trauma3Rojelle LezamaAún no hay calificaciones
- Head Injuries AnaesthesiaDocumento14 páginasHead Injuries AnaesthesiaAndy WijayaAún no hay calificaciones
- Final Online Exam Guideline CBTDocumento105 páginasFinal Online Exam Guideline CBTfaisalaminwani121Aún no hay calificaciones
- Stroke Imaging FINALDocumento90 páginasStroke Imaging FINALChaitanya Jsk100% (1)
- C 1+ 2 Surgicl Pathology of OesophagusDocumento91 páginasC 1+ 2 Surgicl Pathology of OesophagusSayuridark5Aún no hay calificaciones
- Mohd Helmy B Abu Bakar Farrah Hanna BT Mohd Nasir Khairunisa BT JuhariDocumento24 páginasMohd Helmy B Abu Bakar Farrah Hanna BT Mohd Nasir Khairunisa BT Juharimie_anumAún no hay calificaciones
- A Rare Case of Bochdalek Hernia in Adult: A Case ReportDocumento3 páginasA Rare Case of Bochdalek Hernia in Adult: A Case ReportAmbreen FatimaAún no hay calificaciones
- Imaging in Genitourinary SystemDocumento77 páginasImaging in Genitourinary SystemIrvan R. Loho100% (1)
- Prolactinoma1 PDFDocumento30 páginasProlactinoma1 PDFMohammed Younis ShaheenAún no hay calificaciones
- Tethered Spinal Cord SyndromeDocumento7 páginasTethered Spinal Cord SyndromeeditEonAún no hay calificaciones
- Imaging of Orbit and EarDocumento60 páginasImaging of Orbit and Earnila rosalina100% (1)
- Acute Scrotal Swelling & Pain in ChildrenDocumento58 páginasAcute Scrotal Swelling & Pain in ChildrenalaaAún no hay calificaciones
- Ahmad Kurnia: Prediksi, Intervensi, Deteksi Dini Kanker PyudaraDocumento79 páginasAhmad Kurnia: Prediksi, Intervensi, Deteksi Dini Kanker PyudaraTekkhapulephel ParidudinAún no hay calificaciones
- Tumours of The Central Nervous System: FM Brett MD., FrcpathDocumento57 páginasTumours of The Central Nervous System: FM Brett MD., FrcpathDrGasnasAún no hay calificaciones
- Round Cell TumorsDocumento86 páginasRound Cell TumorsMadhura ShekatkarAún no hay calificaciones
- ATLS 8th EditionDocumento50 páginasATLS 8th EditionPaolo VegaAún no hay calificaciones
- Open FractureDocumento106 páginasOpen FractureNizwan ShamAún no hay calificaciones
- 7.30.08 Volk. Mesenteric IschemiaDocumento16 páginas7.30.08 Volk. Mesenteric Ischemiaowcordal7297Aún no hay calificaciones
- Acute Limb Ischemia Vs Critical Limb Ischemia: Clinical PracticeDocumento51 páginasAcute Limb Ischemia Vs Critical Limb Ischemia: Clinical PracticedrhendyjuniorAún no hay calificaciones
- Intradural Extramedullary TumorsDocumento10 páginasIntradural Extramedullary TumorsFaizyab AhmedAún no hay calificaciones
- OPHTHALMOPLEGIADocumento58 páginasOPHTHALMOPLEGIAAryo Handoko SitorusAún no hay calificaciones
- Dr. Kiki - Pengantar Trauma UpdateDocumento20 páginasDr. Kiki - Pengantar Trauma UpdateRsud Malinau Ppk Blud100% (1)
- Jurnal Bedah PPDS (Autosaved)Documento27 páginasJurnal Bedah PPDS (Autosaved)RadenSiwi Bagus Hadhiningrat100% (1)
- Acute AppendicitisDocumento36 páginasAcute AppendicitisOlivia CristieAún no hay calificaciones
- Abdominal ImagingDocumento45 páginasAbdominal ImagingFahriansyah Mp Tmc100% (1)
- Carotid Cavernous Fisstula (CCF)Documento78 páginasCarotid Cavernous Fisstula (CCF)Deny Handayanto0% (1)
- PSGS Review 2015Documento230 páginasPSGS Review 2015yassercarlomanAún no hay calificaciones
- Diagnosis and Management of Infantile HemangiomaDocumento47 páginasDiagnosis and Management of Infantile HemangiomaSteph FergusonAún no hay calificaciones
- 1.initial Assessment in Trauma PatientDocumento50 páginas1.initial Assessment in Trauma PatientLisa Wendi ChachaAún no hay calificaciones
- AMARACHI WORK FinalizedDocumento67 páginasAMARACHI WORK FinalizedocAún no hay calificaciones
- Ventilator Graphics & Trouble-Shooting - EditedDocumento64 páginasVentilator Graphics & Trouble-Shooting - EditedAbhishek SinghAún no hay calificaciones
- Lipo LaserDocumento13 páginasLipo LaserLuis A Gil Pantoja100% (1)
- PMLSDocumento9 páginasPMLSChan ChanAún no hay calificaciones
- BioavailabilityDocumento35 páginasBioavailabilityDr. Bharat JainAún no hay calificaciones
- On and Off Male Birth Control MethodsDocumento2 páginasOn and Off Male Birth Control MethodsLeón L.PAún no hay calificaciones
- Gastroenterology Evaluation TemplateDocumento2 páginasGastroenterology Evaluation Templatee-MedTools88% (8)
- Lesson 3 - Substance Use, Addictions, Mental Health, Stigma and Discrimination and in The WorkplaceDocumento8 páginasLesson 3 - Substance Use, Addictions, Mental Health, Stigma and Discrimination and in The WorkplaceCala WritesAún no hay calificaciones
- Icd9 Icd10 Reference SheetDocumento1 páginaIcd9 Icd10 Reference Sheetapi-272182068Aún no hay calificaciones
- P1 RleDocumento34 páginasP1 RleMary Jean GicaAún no hay calificaciones
- Complications of Insulin TherapyDocumento16 páginasComplications of Insulin TherapyIngrid NicolasAún no hay calificaciones
- Infusion PumpDocumento14 páginasInfusion PumpSREEDEVI T SURESHAún no hay calificaciones
- Vertical Root Fracture !Documento42 páginasVertical Root Fracture !Dr Dithy kkAún no hay calificaciones
- Nursing Nclex 2005Documento39 páginasNursing Nclex 2005Hasan A AsFourAún no hay calificaciones
- Abnormal Vaginal Bleeding Policar 051611Documento69 páginasAbnormal Vaginal Bleeding Policar 051611bidan22Aún no hay calificaciones
- UntitledDocumento17 páginasUntitledInggrid Aprilia ChristyAún no hay calificaciones
- TramadolDocumento2 páginasTramadolJordanne EtisAún no hay calificaciones
- Management Thoracic Pain 2019Documento9 páginasManagement Thoracic Pain 2019Lotte WeggemanAún no hay calificaciones
- Lista Preturi Teste Genetice GendiaDocumento227 páginasLista Preturi Teste Genetice GendiaMatei FloriAún no hay calificaciones
- Grand Case Presentation InformationDocumento7 páginasGrand Case Presentation InformationCristina L. JaysonAún no hay calificaciones
- TORCHDocumento32 páginasTORCHJafar NoryAún no hay calificaciones
- Eye Lids and Lacrimal System: Dr. Binto Akturusiano, SPMDocumento59 páginasEye Lids and Lacrimal System: Dr. Binto Akturusiano, SPMranz ibonkAún no hay calificaciones
- Acadia PharmaceuticalsDocumento3 páginasAcadia PharmaceuticalsAman DecoraterAún no hay calificaciones
- The Apolinario Mabini Syphilis Rumors and Late 19th Century Philippine Power PlayDocumento15 páginasThe Apolinario Mabini Syphilis Rumors and Late 19th Century Philippine Power PlayHaneul KImAún no hay calificaciones
- Detoxification:Management of AmaDocumento3 páginasDetoxification:Management of AmaqueencelAún no hay calificaciones
- Chronic Kidney DiseaseDocumento22 páginasChronic Kidney DiseaseAchmad ZainudinAún no hay calificaciones
- TicksDocumento1 páginaTicksTheChronicleHeraldAún no hay calificaciones
- Textbook of Gynaecological OncologyDocumento58 páginasTextbook of Gynaecological OncologyMarco Vinicio Benavides Osorto100% (2)
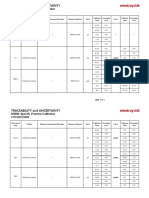
- Specific Proteins Calibrator-150721009-BS600Documento2 páginasSpecific Proteins Calibrator-150721009-BS600S6b2Aún no hay calificaciones