También podría gustarte
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5782)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- 15-09-29 DPREMB ValidityDocumento19 páginas15-09-29 DPREMB ValidityStephen FaraoneAún no hay calificaciones
- Complete Drug StudyDocumento239 páginasComplete Drug StudyRPh Krishna Chandra Jagrit0% (1)
- Meridian Flush Empowerments Levels 3&4 Manual PDFDocumento8 páginasMeridian Flush Empowerments Levels 3&4 Manual PDFJoyce Lozano100% (2)
- User Manual LIS 1050 LT1370 Ing - Rev2Documento27 páginasUser Manual LIS 1050 LT1370 Ing - Rev2AlexeyAún no hay calificaciones
- Review Article: Greco-Arab and Islamic Herbal-Derived Anticancer Modalities: From Tradition To Molecular MechanismsDocumento14 páginasReview Article: Greco-Arab and Islamic Herbal-Derived Anticancer Modalities: From Tradition To Molecular Mechanismsdragan_p2Aún no hay calificaciones
- NAPLEX NoteDocumento58 páginasNAPLEX Notebapimirab654Aún no hay calificaciones
- One Compartment KineticsDocumento31 páginasOne Compartment KineticsAna Francisca100% (1)
- Approach To The Child With AnemiaDocumento9 páginasApproach To The Child With Anemiasack26_11_93Aún no hay calificaciones
- Secondary SyphilisDocumento2 páginasSecondary SyphilisRoberto López MataAún no hay calificaciones
- Michigan Legislative Analysis - SCOPE OF PRACTICE FOR COUNSELORS 2019-HLA-4325-7B3BE14ADocumento5 páginasMichigan Legislative Analysis - SCOPE OF PRACTICE FOR COUNSELORS 2019-HLA-4325-7B3BE14ABeverly TranAún no hay calificaciones
- Dilemma 1Documento6 páginasDilemma 1api-296594594Aún no hay calificaciones
- Discharge PlanDocumento3 páginasDischarge PlanRoberto QuimsonAún no hay calificaciones
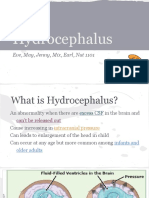
- HydrocephalusDocumento17 páginasHydrocephalusapi-265714286Aún no hay calificaciones
- MedHealthQuestionnaire PDFDocumento2 páginasMedHealthQuestionnaire PDFDonna DominnoAún no hay calificaciones
- Interpersonal Process Recall (IPR) counselling techniqueDocumento8 páginasInterpersonal Process Recall (IPR) counselling techniqueTanmay L. JoshiAún no hay calificaciones
- Anxiety Disorders Lesson PlanDocumento32 páginasAnxiety Disorders Lesson Planapi-284104206Aún no hay calificaciones
- PPPD HandoutDocumento3 páginasPPPD HandoutBryanAún no hay calificaciones
- 24 Doctors With The Courage To Tell The Truth About Distilled WaterDocumento22 páginas24 Doctors With The Courage To Tell The Truth About Distilled WaterEnglishTutr100% (5)
- Management of Unconscious PatientDocumento51 páginasManagement of Unconscious PatientEmenike Donald Ejieji50% (2)
- History of Physiotherapy Profession BibliographyDocumento31 páginasHistory of Physiotherapy Profession BibliographyDr. Krishna N. SharmaAún no hay calificaciones
- Types of Salt Compared: Himalayan vs Kosher vs Sea vs TableDocumento7 páginasTypes of Salt Compared: Himalayan vs Kosher vs Sea vs TableThanabalan MunuswamyAún no hay calificaciones
- HUSNI ADAM - Jurnal Utama No.3Documento3 páginasHUSNI ADAM - Jurnal Utama No.3Adam HusniAún no hay calificaciones
- Etiology Hypertension PDFDocumento2 páginasEtiology Hypertension PDFTrisha100% (1)
- (Methods in Molecular Biology 1149) Alain Filloux, Juan-Luis Ramos (Eds.) - Pseudomonas Methods and Protocols-Humana Press (2014)Documento531 páginas(Methods in Molecular Biology 1149) Alain Filloux, Juan-Luis Ramos (Eds.) - Pseudomonas Methods and Protocols-Humana Press (2014)Muhammad ShakirAún no hay calificaciones
- Schoch 2014Documento35 páginasSchoch 2014Bianca CorreiaAún no hay calificaciones
- Evidence Based Practice, Step by Step Asking The.28Documento4 páginasEvidence Based Practice, Step by Step Asking The.28Putra PurnamaAún no hay calificaciones
- B Cells and T Follicular Helper Cells Mediate Response To Checkpoint Inhibitors in High Mutation Burden Mouse Models of Breast CancerDocumento38 páginasB Cells and T Follicular Helper Cells Mediate Response To Checkpoint Inhibitors in High Mutation Burden Mouse Models of Breast CancerRoger FigueiredoAún no hay calificaciones
- Medicinal Potentials of Semecarpus Anacardiumnut A ReviewDocumento5 páginasMedicinal Potentials of Semecarpus Anacardiumnut A ReviewyigalbyAún no hay calificaciones
- Zanki Renal PathologyDocumento134 páginasZanki Renal Pathologysmian08Aún no hay calificaciones
- Maxillary Anesthetic TechniquesDocumento55 páginasMaxillary Anesthetic TechniquesMera Emad100% (4)