También podría gustarte
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsDe EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsCalificación: 5 de 5 estrellas5/5 (9)
- Pediatric Community Acquired Pneumonia: Dr. Vidal and Dr. VisayaDocumento33 páginasPediatric Community Acquired Pneumonia: Dr. Vidal and Dr. VisayaRenette UyAún no hay calificaciones
- Mark Anthony A. Tom, M.D. First Year Internal Medicine Resident Davao Doctors HospitalDocumento55 páginasMark Anthony A. Tom, M.D. First Year Internal Medicine Resident Davao Doctors HospitalMark Anthony TomAún no hay calificaciones
- PCAP - SummaryDocumento4 páginasPCAP - SummaryNani TumlosAún no hay calificaciones
- PCAP ReportDocumento28 páginasPCAP ReportAngeline Zamoras-ToledoAún no hay calificaciones
- Pneumonia 1 2015Documento2 páginasPneumonia 1 2015Min MawAún no hay calificaciones
- Clinical Practice Guidelines in The Evaluation and Management of PCAPDocumento38 páginasClinical Practice Guidelines in The Evaluation and Management of PCAPJames de Jesus86% (7)
- Pulmonary InfectionsDocumento16 páginasPulmonary InfectionsFawad AhmedAún no hay calificaciones
- Habits Are Some of The Strategies RecommendedDocumento30 páginasHabits Are Some of The Strategies Recommendedmd.dascalescu2486Aún no hay calificaciones
- Pediatrics Community Acquired Pneumonia: Isimijola OpeyemiDocumento30 páginasPediatrics Community Acquired Pneumonia: Isimijola OpeyemiFavourAún no hay calificaciones
- Clinical Management: PGI Eileen Andres PediatricsDocumento9 páginasClinical Management: PGI Eileen Andres PediatricsMichael BonillaAún no hay calificaciones
- PCAP GuidelinesDocumento20 páginasPCAP GuidelinesPatricia Anne Collantes90% (20)
- Pediatric Community Acquired PneumoniaDocumento50 páginasPediatric Community Acquired PneumoniaggalicinaoAún no hay calificaciones
- Infectious Diseases II PDFDocumento62 páginasInfectious Diseases II PDFhuong LAún no hay calificaciones
- Cap Guidelines 2010Documento42 páginasCap Guidelines 2010Marion Andrea PoblacionAún no hay calificaciones
- Neutropenic Fever Empiric TherapyDocumento5 páginasNeutropenic Fever Empiric TherapyRominaPulvermüllerSalvatierraAún no hay calificaciones
- Case Studies of Lower Respiratory Tract InfectionsDocumento25 páginasCase Studies of Lower Respiratory Tract InfectionsMarianAún no hay calificaciones
- PCAP GuidelinesDocumento15 páginasPCAP GuidelinesQueenie CuaroAún no hay calificaciones
- When Your Patient Has PneumoniaDocumento4 páginasWhen Your Patient Has PneumoniaawuahbohAún no hay calificaciones
- BCCA Febrile Neutropenia GuidelinesDocumento2 páginasBCCA Febrile Neutropenia GuidelinesdenokayuMRAún no hay calificaciones
- BPS Oncology Pharmacy Practice ExamDocumento11 páginasBPS Oncology Pharmacy Practice Examiman100% (3)
- Management of Adult Febrile Neutropenia: 15011500-10123 99 Street Edmonton, Alberta T5J 3H1Documento4 páginasManagement of Adult Febrile Neutropenia: 15011500-10123 99 Street Edmonton, Alberta T5J 3H1Tio Prima SAún no hay calificaciones
- Anesthaesia and Intensive CareDocumento139 páginasAnesthaesia and Intensive CareIvan Kurniadi100% (2)
- Protocols Sepsis Treatment Stony BrookDocumento6 páginasProtocols Sepsis Treatment Stony BrookVicky Chrystine SianiparAún no hay calificaciones
- Management of CAP: Recent Guideline in Daily PractisDocumento38 páginasManagement of CAP: Recent Guideline in Daily PractisNila hermawatiAún no hay calificaciones
- Anaesthesia & Intensive Care: For Fcai, Frca EdaicDocumento139 páginasAnaesthesia & Intensive Care: For Fcai, Frca EdaicMuhammad Farid100% (1)
- Day 1 Biomedis UAP Sepsis - MontoyaDocumento45 páginasDay 1 Biomedis UAP Sepsis - MontoyaRye CalderonAún no hay calificaciones
- Pneumonia GuidelinesDocumento4 páginasPneumonia GuidelinesFatkhul Ali ImronAún no hay calificaciones
- Antibiotic Guidelines Elderly UTI Rationale C Diff & PID Amended 15.09.11 UTI & Flu Amended 04.10 OM Ref 11.11Documento29 páginasAntibiotic Guidelines Elderly UTI Rationale C Diff & PID Amended 15.09.11 UTI & Flu Amended 04.10 OM Ref 11.11Syed Yasir HusainAún no hay calificaciones
- I and I MODULE INFECTIOUS DISORDERSDocumento23 páginasI and I MODULE INFECTIOUS DISORDERSJeffrey GazmenAún no hay calificaciones
- I and I Module Infectious DisordersDocumento23 páginasI and I Module Infectious DisordersCaitlynAún no hay calificaciones
- Cap CPGDocumento40 páginasCap CPGMary Joy Oros-VallejeraAún no hay calificaciones
- Pneumonia: Recent Evidence Based UpdatesDocumento30 páginasPneumonia: Recent Evidence Based UpdatesAli AzamAún no hay calificaciones
- Antibiotic RespirDocumento2 páginasAntibiotic Respirlaur_rbAún no hay calificaciones
- Bcps Preparatory Class On Pediatrics: Saba Javed HussainDocumento65 páginasBcps Preparatory Class On Pediatrics: Saba Javed HussainSyahrul Tuba Al FatihAún no hay calificaciones
- Respiratory SlidesDocumento40 páginasRespiratory SlidesmaheshAún no hay calificaciones
- Community Acquired PneumoniaDocumento37 páginasCommunity Acquired PneumoniaJoean CabarlocAún no hay calificaciones
- Penatalaksanaan CAPDocumento31 páginasPenatalaksanaan CAPushagi-chanAún no hay calificaciones
- Screenshot 2020-03-20 at 08.25.44 PDFDocumento10 páginasScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresAún no hay calificaciones
- Lower Respiratory Tract Infection - CAP: Therapy II - LabDocumento14 páginasLower Respiratory Tract Infection - CAP: Therapy II - Labsameh EidAún no hay calificaciones
- MS OR Sunday1to100Documento14 páginasMS OR Sunday1to100Ramon Carlo AlmiranezAún no hay calificaciones
- CC Junsay Nicole Xyza T. Learning Interaction FormDocumento10 páginasCC Junsay Nicole Xyza T. Learning Interaction FormNicole Xyza JunsayAún no hay calificaciones
- Pca PP Revised 6 4 14 v6Documento12 páginasPca PP Revised 6 4 14 v6api-244230664Aún no hay calificaciones
- Diagnosis and Management of Febrile Neutropenia 4567Documento6 páginasDiagnosis and Management of Febrile Neutropenia 4567Hisham ElhadidiAún no hay calificaciones
- Respiratory Medicine 1 50Documento33 páginasRespiratory Medicine 1 50Ahmed Kh. Abu WardaAún no hay calificaciones
- Drug Study OrthoDocumento17 páginasDrug Study OrthoMc Crister SilangAún no hay calificaciones
- PCAP Report ClerkshipDocumento54 páginasPCAP Report ClerkshipMichelleAquinoSuzukiAún no hay calificaciones
- Clinical Practice Guideline On Neonatal Sepsis: Summarized by Dr. Catherine Chua October 2012Documento3 páginasClinical Practice Guideline On Neonatal Sepsis: Summarized by Dr. Catherine Chua October 2012Joey CuayoAún no hay calificaciones
- FeverDocumento27 páginasFeverTilaye GebruAún no hay calificaciones
- Pediatric PneumoniaDocumento58 páginasPediatric PneumoniaJohn Christopher LucesAún no hay calificaciones
- Acute Respiratory Distress SyndromeDocumento4 páginasAcute Respiratory Distress SyndromeBianca WelchAún no hay calificaciones
- Pediatric Community-Acquired Pneumonia: CC Trisha Pamela OquendoDocumento70 páginasPediatric Community-Acquired Pneumonia: CC Trisha Pamela OquendoJessa MaeAún no hay calificaciones
- Febrile Neonate Clinical Practice Guideline: CatheterizedDocumento1 páginaFebrile Neonate Clinical Practice Guideline: Catheterizedromeoenny4154Aún no hay calificaciones
- Diagnosis & Treatment of Healthcare-Associated Pneumonia: Beyond The GuidelineDocumento57 páginasDiagnosis & Treatment of Healthcare-Associated Pneumonia: Beyond The GuidelineKei MiyazakiAún no hay calificaciones
- Pneumonias UpToDateDocumento52 páginasPneumonias UpToDateHEBA NAJJARAún no hay calificaciones
- Nsg6430 Final Exam ReviewDocumento10 páginasNsg6430 Final Exam ReviewJOKAAún no hay calificaciones
- CAP CURB-65 GuidelinesDocumento1 páginaCAP CURB-65 GuidelinesAndy LoakAún no hay calificaciones
- Andi PosterDocumento10 páginasAndi PosterChijioke Chioli PascalAún no hay calificaciones
- Stroke Management Clinical Practice GuidelinesDocumento26 páginasStroke Management Clinical Practice GuidelinesprinsepejesseAún no hay calificaciones
- TASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)Documento2 páginasTASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)ጉራማይሌ TubeAún no hay calificaciones
- 2011 Blood TransfusionDocumento6 páginas2011 Blood TransfusionJeanne Mae Lee AfallaAún no hay calificaciones
- AnaphylaxisDocumento5 páginasAnaphylaxisJeanne Mae Lee AfallaAún no hay calificaciones
- EBM Probiotics For BacvagDocumento12 páginasEBM Probiotics For BacvagJeanne Mae Lee AfallaAún no hay calificaciones
- Journal Ent July Dec 2014 SupplementDocumento16 páginasJournal Ent July Dec 2014 SupplementJeanne Mae Lee AfallaAún no hay calificaciones
- Fungus PDFDocumento4 páginasFungus PDFPrashant MishraAún no hay calificaciones
- Piece of The PuzzleDocumento18 páginasPiece of The PuzzleJeanne Mae Lee AfallaAún no hay calificaciones
- PowerNote 2013Documento42 páginasPowerNote 2013Jeanne Mae Lee AfallaAún no hay calificaciones
- Collection of Blood From DonorsDocumento7 páginasCollection of Blood From DonorsBernardoHernandezAún no hay calificaciones
- BCC, Laboratory Specimens and Microscopy, MLT 1040, FINAL EXAM GRADEDocumento24 páginasBCC, Laboratory Specimens and Microscopy, MLT 1040, FINAL EXAM GRADEalphacetaAún no hay calificaciones
- HKDSE Biology Part 3 Health & DiseasesDocumento17 páginasHKDSE Biology Part 3 Health & DiseasesTSZ YAN CHEUNGAún no hay calificaciones
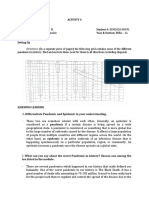
- Activity in MathDocumento26 páginasActivity in MathAlyson GregorioAún no hay calificaciones
- Epidemiological Investigation On Parasitic Diseases of Buffaloes (Bubalus Bubalis) in Kurigram District of BangladeshDocumento77 páginasEpidemiological Investigation On Parasitic Diseases of Buffaloes (Bubalus Bubalis) in Kurigram District of BangladeshMamunpara100% (1)
- Kami Export - Pathogens-Stations-ReviewDocumento3 páginasKami Export - Pathogens-Stations-ReviewAshley Cervantes VillanuevaAún no hay calificaciones
- ImpetigoDocumento11 páginasImpetigoShailendra RijalAún no hay calificaciones
- 1 WhydowefallillDocumento9 páginas1 WhydowefallillAbhimanyu BahreeAún no hay calificaciones
- 13fk10 Hav Igg-Igm (D) Ins (En) CeDocumento2 páginas13fk10 Hav Igg-Igm (D) Ins (En) CeCrcrjhjh RcrcjhjhAún no hay calificaciones
- Hepatites 1Documento49 páginasHepatites 1Milan JavornikAún no hay calificaciones
- Pneumococcus ExpertRules V3.2 20190613Documento3 páginasPneumococcus ExpertRules V3.2 20190613Julyadharma Wangsa DharmaAún no hay calificaciones
- Stool Analysis and Other Body Fluid AnalysisDocumento51 páginasStool Analysis and Other Body Fluid AnalysisPutri Senna Rahayu100% (2)
- Icd 10Documento1 páginaIcd 10renatanurulAún no hay calificaciones
- Ref - Complete Notes PDFDocumento101 páginasRef - Complete Notes PDFMary Rose AudienciaAún no hay calificaciones
- (MICRO2) Gram Negative CocciDocumento41 páginas(MICRO2) Gram Negative CocciMadhu MithaAún no hay calificaciones
- PositioningDocumento97 páginasPositioningzixdiddy100% (1)
- AIDS Is Not InfectiousDocumento18 páginasAIDS Is Not Infectiousbadboy6.868510Aún no hay calificaciones
- MCQs For LaboratoryDocumento42 páginasMCQs For Laboratorynarendrakumar94100% (1)
- Perioperative NursingDocumento13 páginasPerioperative NursingTobiDaAún no hay calificaciones
- Question: 1 of 100 / Overall Score: 80%: True / FalseDocumento84 páginasQuestion: 1 of 100 / Overall Score: 80%: True / FalseGalaleldin AliAún no hay calificaciones
- EndophthalmitisDocumento36 páginasEndophthalmitisHieLdaJanuariaAún no hay calificaciones
- Infection and Immunity Bacterial, Viral and FungalDocumento30 páginasInfection and Immunity Bacterial, Viral and FungalCharrieBognotRagadiAún no hay calificaciones
- Canine Parvovirus Infection in DogsDocumento2 páginasCanine Parvovirus Infection in DogsCharly Lab GumbleAún no hay calificaciones
- Medical Entomology: - Definition - History - Intro To Arthropods and Insects - Intro To Vector-Borne Disease ConceptsDocumento58 páginasMedical Entomology: - Definition - History - Intro To Arthropods and Insects - Intro To Vector-Borne Disease ConceptsPipi Montok100% (1)
- 11 Forrest The Investigation of ElectromedicineDocumento70 páginas11 Forrest The Investigation of ElectromedicineMatthias WeisserAún no hay calificaciones
- MCQ's With KEY Medicine - BDocumento8 páginasMCQ's With KEY Medicine - BSiraj Ul IslamAún no hay calificaciones
- 2008 01 10 BDocumento10 páginas2008 01 10 BSouthern Maryland OnlineAún no hay calificaciones
- Subject PredicateDocumento69 páginasSubject PredicateyuldaAún no hay calificaciones
- Test Your Organisation With The 12-Boxes FrameworkDocumento64 páginasTest Your Organisation With The 12-Boxes FrameworkOxfamAún no hay calificaciones
- DNA ReplicationDocumento5 páginasDNA Replicationvijayalakshmiraman100% (1)