También podría gustarte
- Somatosensory Teachers Manual: for Somatosensory Science FactsDe EverandSomatosensory Teachers Manual: for Somatosensory Science FactsAún no hay calificaciones
- TZS Sympathietic and Parasympathetic NS 2018Documento31 páginasTZS Sympathietic and Parasympathetic NS 2018poopziAún no hay calificaciones
- Light and Electron Microscopy of Cells and TissuesDe EverandLight and Electron Microscopy of Cells and TissuesAún no hay calificaciones
- Added To Autonomic PhysiologyDocumento4 páginasAdded To Autonomic Physiologymahmoud ezzeldeenAún no hay calificaciones
- 8 - Cerebellum, Diencephalon, Basal NucleiDocumento60 páginas8 - Cerebellum, Diencephalon, Basal Nucleib.ozyurek84Aún no hay calificaciones
- Autonomic Nervous System-1Documento46 páginasAutonomic Nervous System-1a-tldAún no hay calificaciones
- CerebellumDocumento28 páginasCerebellumZoya MoraniAún no hay calificaciones
- Physiology of Motor TractsDocumento29 páginasPhysiology of Motor Tractsrj100% (1)
- CNS 10 MarksDocumento12 páginasCNS 10 Marksnico diangeloAún no hay calificaciones
- CNS Special Sense, ReproDocumento52 páginasCNS Special Sense, ReproihavetallbrainsAún no hay calificaciones
- Basal Ganglia ModifiedDocumento34 páginasBasal Ganglia ModifiedNada MohammedAún no hay calificaciones
- The Autonomic System 2019Documento50 páginasThe Autonomic System 2019TheBoss 20Aún no hay calificaciones
- 2-Long Ascending TractsDocumento27 páginas2-Long Ascending Tractsyaram3512Aún no hay calificaciones
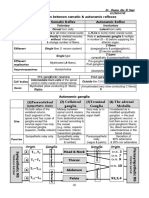
- ANS TablesDocumento4 páginasANS Tablesahmed yousefAún no hay calificaciones
- Autonomic Nervous SystemDocumento57 páginasAutonomic Nervous SystemGeremew SiyumAún no hay calificaciones
- Topic 2: The Extrapyramidal System. The CerebellumDocumento42 páginasTopic 2: The Extrapyramidal System. The Cerebellumprashant singhAún no hay calificaciones
- ThalamusDocumento17 páginasThalamusPrafulla KasarAún no hay calificaciones
- Basal GangliaDocumento28 páginasBasal GangliaK SAún no hay calificaciones
- Lecture 1 Introduction & General Features of Nervous SystemDocumento28 páginasLecture 1 Introduction & General Features of Nervous Systemdaw022Aún no hay calificaciones
- Spinal CordDocumento50 páginasSpinal CordReem 10Aún no hay calificaciones
- CerebellumDocumento36 páginasCerebellumsaskiabpAún no hay calificaciones
- Cerebral Cortex Cerebral CortexDocumento62 páginasCerebral Cortex Cerebral CortexMORGAN LAMBERTAún no hay calificaciones
- Motor II: Central MechanismsDocumento40 páginasMotor II: Central MechanismsKalil MenezesAún no hay calificaciones
- Intergrated Clinical Case Discussion - Stroke 2020Documento66 páginasIntergrated Clinical Case Discussion - Stroke 2020Sabashnee GovenderAún no hay calificaciones
- Decending and Ascending Tracts - Eve - 14-Oct-2022Documento29 páginasDecending and Ascending Tracts - Eve - 14-Oct-2022Pyaesone AungAún no hay calificaciones
- 3.1 - Ii Reward System 05-09-2023Documento81 páginas3.1 - Ii Reward System 05-09-2023Talha TariqAún no hay calificaciones
- Spinal Cord Injury Garstang 10-16-09 GrayscaleDocumento12 páginasSpinal Cord Injury Garstang 10-16-09 GrayscaleJayAún no hay calificaciones
- The Central Nervous System: Andi AnsharullahDocumento60 páginasThe Central Nervous System: Andi AnsharullahAnonymous vUl83IptiSAún no hay calificaciones
- Examination of Nervous System - BasicsDocumento93 páginasExamination of Nervous System - BasicsAniq Zahran MasomAún no hay calificaciones
- Cell PhysiologyDocumento2 páginasCell PhysiologyQuang NguyenAún no hay calificaciones
- The 2 Lecture Today: Structure and Connections of The Basal Ganglia. Motor Pathways Arising From The Brain StemDocumento34 páginasThe 2 Lecture Today: Structure and Connections of The Basal Ganglia. Motor Pathways Arising From The Brain StemJimach Bol WieAún no hay calificaciones
- NeuroscienceDocumento5 páginasNeuroscienceChing MacarubboAún no hay calificaciones
- k2 Neuroanatomy of The Musculo-Skeletal Disorders-2016Documento85 páginask2 Neuroanatomy of The Musculo-Skeletal Disorders-2016icha100% (1)
- Neurobiology of SleepDocumento38 páginasNeurobiology of SleepSwayang Sudha PandaAún no hay calificaciones
- Cerebellum DR SanyamandweDocumento31 páginasCerebellum DR SanyamandweTinashe MatomboAún no hay calificaciones
- Brain Anatomy: CerebellumDocumento31 páginasBrain Anatomy: Cerebellumdr_mohanadAún no hay calificaciones
- Histology of The Spinal Cord, Nerve, Sensory and Vegetative GangliaDocumento23 páginasHistology of The Spinal Cord, Nerve, Sensory and Vegetative Gangliashmirtb100% (2)
- Nutshell NeuroDocumento15 páginasNutshell NeuroAdeel abbas rajaAún no hay calificaciones
- Cerebral Cortex Cerebral CortexDocumento62 páginasCerebral Cortex Cerebral CortexJ NAún no hay calificaciones
- Lecture (17) Basal GangliaDocumento13 páginasLecture (17) Basal GangliaAkashAún no hay calificaciones
- Introduction To AnsDocumento12 páginasIntroduction To AnsSusmita BeheraAún no hay calificaciones
- Autonomic Pharmacology: OutlineDocumento9 páginasAutonomic Pharmacology: OutlineEryll Paolo AleaAún no hay calificaciones
- Internal CapsuleDocumento25 páginasInternal CapsuleMadan KumarAún no hay calificaciones
- Proprioceptive Sensory SystemsDocumento9 páginasProprioceptive Sensory SystemsRex HuangAún no hay calificaciones
- Basic Concepts in Neuro-PhysiologyDocumento19 páginasBasic Concepts in Neuro-Physiologymuhammad sadiqAún no hay calificaciones
- DR - Mohammad Al-Salem Parrt Summary: 1 Amal Saeed OdehDocumento178 páginasDR - Mohammad Al-Salem Parrt Summary: 1 Amal Saeed Odehk8rbwkpgn7Aún no hay calificaciones
- Basal Ganglia: Dr. Mohamed AlzainDocumento53 páginasBasal Ganglia: Dr. Mohamed AlzainAva EbsAún no hay calificaciones
- 3 CNS PDFDocumento42 páginas3 CNS PDFPutriAún no hay calificaciones
- Basal Ganglia: Dr. Israa M. Sulaiman Department of Anatomy Ims/MsuDocumento60 páginasBasal Ganglia: Dr. Israa M. Sulaiman Department of Anatomy Ims/Msuadelina.jianu9991Aún no hay calificaciones
- Coordination of Movement-Lecture Notes 20201Documento47 páginasCoordination of Movement-Lecture Notes 20201Zobayer AhmedAún no hay calificaciones
- Lesions of Motor System Lesions of Motor System: Professor Hayder K.HassounDocumento17 páginasLesions of Motor System Lesions of Motor System: Professor Hayder K.HassounAhmeed SafaaAún no hay calificaciones
- Basal Ganglia (BG) : Purves Chapter 18Documento35 páginasBasal Ganglia (BG) : Purves Chapter 18Addison FreemanAún no hay calificaciones
- Sensory SystemDocumento101 páginasSensory Systemsalmankhan09215Aún no hay calificaciones
- Cranial NervesDocumento14 páginasCranial NervesAdrija ChatterjeeAún no hay calificaciones
- Autonomic Nervous System: Rodina Rivera-Gorospe, M.DDocumento44 páginasAutonomic Nervous System: Rodina Rivera-Gorospe, M.DPogo LocoAún no hay calificaciones
- Hacks Final FormattedDocumento183 páginasHacks Final Formattedbhoj RAJAún no hay calificaciones
- Neuroscience ReviewDocumento86 páginasNeuroscience ReviewKelly T.Aún no hay calificaciones
- Neuro Part 1 NotesDocumento3 páginasNeuro Part 1 NotesMarc JasminAún no hay calificaciones
- Motoric System: Anggraeni Janar WulanDocumento44 páginasMotoric System: Anggraeni Janar WulanNadiarosmaliaAún no hay calificaciones
- Basal Ganglia & CerebellumDocumento77 páginasBasal Ganglia & Cerebellumyasrul izadAún no hay calificaciones
- DTRDocumento12 páginasDTRZoya MoraniAún no hay calificaciones
- Examination of Lower LimbDocumento18 páginasExamination of Lower LimbZoya MoraniAún no hay calificaciones
- Icm Course Syllabus PDFDocumento8 páginasIcm Course Syllabus PDFZoya Morani100% (1)
- Vital RecordingsDocumento27 páginasVital RecordingsZoya MoraniAún no hay calificaciones
- Introduction To Clinical MedicineDocumento26 páginasIntroduction To Clinical MedicineZoya Morani100% (3)
- Hand DeformityDocumento7 páginasHand DeformityZoya MoraniAún no hay calificaciones
- Inspection - Visual Acuity - Visual Fields - Pupillary Response - Fundoscopic ExamDocumento34 páginasInspection - Visual Acuity - Visual Fields - Pupillary Response - Fundoscopic ExamZoya MoraniAún no hay calificaciones
- Examination of Upper LimbDocumento6 páginasExamination of Upper LimbZoya MoraniAún no hay calificaciones
- CerebrumDocumento45 páginasCerebrumZoya MoraniAún no hay calificaciones
- l8 - End of Life Issues (Part 1)Documento57 páginasl8 - End of Life Issues (Part 1)Zoya MoraniAún no hay calificaciones
- Body Fluid DistributionDocumento56 páginasBody Fluid DistributionZoya Morani100% (1)
- White MatterDocumento19 páginasWhite MatterZoya MoraniAún no hay calificaciones
- 9 ThalamusDocumento10 páginas9 ThalamusZoya MoraniAún no hay calificaciones
- The Movement of Fluid Across The Plasma MembraneDocumento33 páginasThe Movement of Fluid Across The Plasma MembraneZoya MoraniAún no hay calificaciones
- Blood Suppy of BrainDocumento54 páginasBlood Suppy of BrainZoya MoraniAún no hay calificaciones
- Containg Sulfer MetabolismDocumento27 páginasContaing Sulfer MetabolismZoya MoraniAún no hay calificaciones
- MTH100Documento3 páginasMTH100Syed Abdul Mussaver ShahAún no hay calificaciones
- Prestige Institute of Management & Research: Guided By:-Submitted By: - Prof. Arpit Loya Sumeet RattanDocumento21 páginasPrestige Institute of Management & Research: Guided By:-Submitted By: - Prof. Arpit Loya Sumeet RattanSumeet700005Aún no hay calificaciones
- AKI in ChildrenDocumento43 páginasAKI in ChildrenYonas AwgichewAún no hay calificaciones
- Module 4 Active Faults and Other Earthquake Sources: Learning OutcomeDocumento3 páginasModule 4 Active Faults and Other Earthquake Sources: Learning OutcomeFatima Ybanez Mahilum-LimbagaAún no hay calificaciones
- Middle Range Theory Ellen D. Schulzt: Modeling and Role Modeling Katharine Kolcaba: Comfort TheoryDocumento22 páginasMiddle Range Theory Ellen D. Schulzt: Modeling and Role Modeling Katharine Kolcaba: Comfort TheoryMerlinAún no hay calificaciones
- Nissan Copper LTDDocumento11 páginasNissan Copper LTDankit_shahAún no hay calificaciones
- Faa Registry: N-Number Inquiry ResultsDocumento3 páginasFaa Registry: N-Number Inquiry Resultsolga duqueAún no hay calificaciones
- Provision of EPCI Services For EPCIC Sidayu Wellhead Platforms and Pipelines Sidayu Field DevelopmentDocumento7 páginasProvision of EPCI Services For EPCIC Sidayu Wellhead Platforms and Pipelines Sidayu Field Developmentriandi100% (1)
- Surface TensionDocumento13 páginasSurface TensionElizebeth GAún no hay calificaciones
- Logic NotesDocumento19 páginasLogic NotesCielo PulmaAún no hay calificaciones
- Bhil Tribal Mobilisation in AlirajpurDocumento14 páginasBhil Tribal Mobilisation in Alirajpurrahul banerjeeAún no hay calificaciones
- Rail Vehicle DynamicsDocumento55 páginasRail Vehicle DynamicsdfAún no hay calificaciones
- Gamak MotorDocumento34 páginasGamak MotorCengiz Sezer100% (1)
- GP1 Q1 Week-1Documento18 páginasGP1 Q1 Week-1kickyknacksAún no hay calificaciones
- Percent by VolumeDocumento19 páginasPercent by VolumeSabrina LavegaAún no hay calificaciones
- Oil Whirl and Whip Instabilities - Within Journal BearingsDocumento27 páginasOil Whirl and Whip Instabilities - Within Journal BearingsTalha AamirAún no hay calificaciones
- Soldier of Fortune PDFDocumento208 páginasSoldier of Fortune PDFNixel SpielAún no hay calificaciones
- 12 Key Principles On Bhava AnalysisDocumento28 páginas12 Key Principles On Bhava AnalysisDhineshAún no hay calificaciones
- Biophoton RevolutionDocumento3 páginasBiophoton RevolutionVyavasayaha Anita BusicAún no hay calificaciones
- Honeycomb Kevlar 49 (Hexcel)Documento3 páginasHoneycomb Kevlar 49 (Hexcel)Julia GarciaAún no hay calificaciones
- Arbor APS STT Unit 01 Design Basics 25 Jan2018Documento31 páginasArbor APS STT Unit 01 Design Basics 25 Jan2018masterlinh2008Aún no hay calificaciones
- Implicit Explicit SignalsDocumento8 páginasImplicit Explicit SignalsVersoza Nel100% (2)
- Basic Geriatric Nursing 6th Edition Williams Test BankDocumento10 páginasBasic Geriatric Nursing 6th Edition Williams Test Bankmaryrodriguezxsntrogkwd100% (49)
- Inferring The Speaker's Tone, ModeDocumento31 páginasInferring The Speaker's Tone, Modeblessilda.delaramaAún no hay calificaciones
- Plans PDFDocumento49 páginasPlans PDFEstevam Gomes de Azevedo85% (34)
- Gypsum Plasterboard: National Standard of The People'S Republic of ChinaDocumento15 páginasGypsum Plasterboard: National Standard of The People'S Republic of ChinaGarry100% (2)
- Semi Finals in Tle 2015Documento3 páginasSemi Finals in Tle 2015LoraineTenorioAún no hay calificaciones
- Course Registration SlipDocumento2 páginasCourse Registration SlipMics EntertainmentAún no hay calificaciones
- 2022 Audi e Tron 22Documento318 páginas2022 Audi e Tron 22Alejandro Alberto Robalino MendezAún no hay calificaciones
- 14p-220 Mud PumpDocumento2 páginas14p-220 Mud PumpMurali Sambandan50% (2)