También podría gustarte
- Roleof Diabetesin ProsthodonticsDocumento4 páginasRoleof Diabetesin ProsthodonticsHemiya ThomasAún no hay calificaciones
- Safety in Manufacturing: Ergonomics: Awkward PosturesDocumento2 páginasSafety in Manufacturing: Ergonomics: Awkward PosturesprashanthAún no hay calificaciones
- Coronoplasty: January 2021Documento14 páginasCoronoplasty: January 2021khalisha salsabila100% (1)
- Impression For Complete Denture1Documento94 páginasImpression For Complete Denture1samar yousif mohamedAún no hay calificaciones
- Extraction: Department of Oral and Maxillofacial SurgeryDocumento26 páginasExtraction: Department of Oral and Maxillofacial SurgerySudip ChakrabortyAún no hay calificaciones
- Imaging in Periodontics PerioDocumento49 páginasImaging in Periodontics PerioFourthMolar.comAún no hay calificaciones
- MCQs on Defence Audit Code Chapter 9 and 10Documento2 páginasMCQs on Defence Audit Code Chapter 9 and 10Rustam SalamAún no hay calificaciones
- LD Certificate and AcknowledgementDocumento5 páginasLD Certificate and Acknowledgementsai thesisAún no hay calificaciones
- The Role of Saliva in ProsthodonticsDocumento84 páginasThe Role of Saliva in ProsthodonticsVidya SenthuAún no hay calificaciones
- Dental Abscess and InfectionsDocumento24 páginasDental Abscess and InfectionsNiyonsaba jean claudeAún no hay calificaciones
- Maxillary Nerve: Dr. Sanjana Mall Department of PedodonticsDocumento48 páginasMaxillary Nerve: Dr. Sanjana Mall Department of PedodonticsSanjana MallAún no hay calificaciones
- Tooth Eruption & Shedding MechanismsDocumento18 páginasTooth Eruption & Shedding MechanismsAnamika PandeyAún no hay calificaciones
- Tooth Eruption and Shedding ExplainedDocumento29 páginasTooth Eruption and Shedding Explainedjenny girl100% (1)
- Components of Removable Partial Denture Prostheses-Dr - PaulamiDocumento35 páginasComponents of Removable Partial Denture Prostheses-Dr - PaulamiVincent SerAún no hay calificaciones
- Endodontic Case Presentation: Ahmad S. AlqahtaniDocumento35 páginasEndodontic Case Presentation: Ahmad S. AlqahtaniVinisha Vipin SharmaAún no hay calificaciones
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionDe EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionAún no hay calificaciones
- Math30.CA U1l1 PolynomialFunctionsDocumento20 páginasMath30.CA U1l1 PolynomialFunctionsUnozxcv Doszxc100% (1)
- PERIO 1. Introduction Part 1Documento69 páginasPERIO 1. Introduction Part 1jpatel24Aún no hay calificaciones
- Bone Grafting Techniques for Maxillary ImplantsDe EverandBone Grafting Techniques for Maxillary ImplantsAún no hay calificaciones
- Maxillary Sinus (NXPowerLite) .PPT / Orthodontic Courses by Indian Dental AcademyDocumento18 páginasMaxillary Sinus (NXPowerLite) .PPT / Orthodontic Courses by Indian Dental Academyindian dental academyAún no hay calificaciones
- RPD Impression ModifiedDocumento27 páginasRPD Impression ModifiedPrince AhmedAún no hay calificaciones
- CHAP 10 Dental Calculus SelfDocumento38 páginasCHAP 10 Dental Calculus SelfarshmeentariqAún no hay calificaciones
- A Large Rhinolith and Importance of Nasal Endoscopy: A Case ReportDocumento3 páginasA Large Rhinolith and Importance of Nasal Endoscopy: A Case ReportIOSRjournalAún no hay calificaciones
- Mandibular Left First Premolar With Two Roots: A Morphological OddityDocumento3 páginasMandibular Left First Premolar With Two Roots: A Morphological OddityAmee PatelAún no hay calificaciones
- RPD ImpressionDocumento49 páginasRPD ImpressionAmar Bimavarapu0% (1)
- Diagnosis ClassDocumento63 páginasDiagnosis ClassRiham AliAún no hay calificaciones
- Fiber Reinforced CompositeDocumento5 páginasFiber Reinforced Compositejcali06Aún no hay calificaciones
- Compomers HistoryDocumento2 páginasCompomers HistoryrojAún no hay calificaciones
- Defence Mechanism of Gingiva PerioDocumento58 páginasDefence Mechanism of Gingiva PerioFourthMolar.com100% (1)
- Geriatric Restorative CareDocumento12 páginasGeriatric Restorative CareCeza CezaaAún no hay calificaciones
- Fragiskos's Oral - Surgery (2007)Documento6 páginasFragiskos's Oral - Surgery (2007)Stanley Santosa KamadjajaAún no hay calificaciones
- Gingival Enlargement: Drg. Ade Ismail A. K.,MDSCDocumento31 páginasGingival Enlargement: Drg. Ade Ismail A. K.,MDSCFina AkmaliaAún no hay calificaciones
- Smoking and PeriodontiumDocumento81 páginasSmoking and Periodontiumanshum guptaAún no hay calificaciones
- Development of TeethDocumento127 páginasDevelopment of Teethdentistpro.orgAún no hay calificaciones
- Cements, Bases and LinersDocumento6 páginasCements, Bases and LinerselsokaryAún no hay calificaciones
- Impressions for Fixed Partial DenturesDocumento53 páginasImpressions for Fixed Partial DenturespragatiAún no hay calificaciones
- Dentin Hypersensitivity2 PDFDocumento5 páginasDentin Hypersensitivity2 PDFIvan TerresAún no hay calificaciones
- Edentulous Patient Exam, Diagnosis and Treatment PlanningDocumento73 páginasEdentulous Patient Exam, Diagnosis and Treatment PlanningMohamedAún no hay calificaciones
- Diseases of The PulpDocumento93 páginasDiseases of The PulpIsha MalabedAún no hay calificaciones
- Fundamentals of Tooth PreparationDocumento6 páginasFundamentals of Tooth PreparationAnamika PandeyAún no hay calificaciones
- Ultrasonic Periodontal DebridementDocumento9 páginasUltrasonic Periodontal DebridementAsus AsusAún no hay calificaciones
- Difference Between Primary and Permanent TeethDocumento17 páginasDifference Between Primary and Permanent TeethMohd Tauseef Khan100% (1)
- Mandibular NerveDocumento8 páginasMandibular NerveSridevi KAún no hay calificaciones
- Mucogingival SurgeryDocumento53 páginasMucogingival SurgeryAbhijeet Shete100% (3)
- Cementum EhtishamDocumento102 páginasCementum EhtishamHannasa R JAún no hay calificaciones
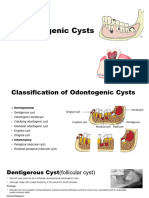
- Odontogenic CystDocumento16 páginasOdontogenic CystMahsaAún no hay calificaciones
- Cysts of The Oral RegionDocumento5 páginasCysts of The Oral RegionPaul Anthony Garcia ConcepcionAún no hay calificaciones
- Basic TxPlanning-Prognosis and Treatment Planning-Revised 9 September 2014Documento54 páginasBasic TxPlanning-Prognosis and Treatment Planning-Revised 9 September 2014DraspiAún no hay calificaciones
- Oral Manifestations of Abused Complete Denture UsageDocumento53 páginasOral Manifestations of Abused Complete Denture UsageBharanija100% (2)
- Behavior ManagementDocumento99 páginasBehavior ManagementMeera SAún no hay calificaciones
- Gingivitis & PeriodontitisDocumento24 páginasGingivitis & PeriodontitisHafid Nur ArzanudinAún no hay calificaciones
- Tests For Biocompatibility of Dental MaterialsDocumento151 páginasTests For Biocompatibility of Dental MaterialsDevanshi SharmaAún no hay calificaciones
- Spread of Oral Infections in Fascial SpacesDocumento69 páginasSpread of Oral Infections in Fascial SpacesMoola Bharath Reddy100% (7)
- Chemical Plaque ControlDocumento37 páginasChemical Plaque ControlHana FikriAún no hay calificaciones
- Posterior Palatal Seal Prostho 1 (EDocFind - Com) (1) 11Documento64 páginasPosterior Palatal Seal Prostho 1 (EDocFind - Com) (1) 11Pranshu TripathiAún no hay calificaciones
- Dentin Hypersensitivity: Understanding the Mechanism and ManagementDocumento4 páginasDentin Hypersensitivity: Understanding the Mechanism and Managementmohamed saadAún no hay calificaciones
- Saliva and Its Prosthodontic Implications / Orthodontic Courses by Indian Dental AcademyDocumento38 páginasSaliva and Its Prosthodontic Implications / Orthodontic Courses by Indian Dental Academyindian dental academyAún no hay calificaciones
- Mandibular Nerve, Chorda Tympani Nerve, Otic GanglionDocumento33 páginasMandibular Nerve, Chorda Tympani Nerve, Otic Ganglionwaniya irumAún no hay calificaciones
- Defense Mechanism of GingivaDocumento46 páginasDefense Mechanism of GingivaSunny MaviAún no hay calificaciones
- Maintaining Stability of Complete DenturesDocumento21 páginasMaintaining Stability of Complete DenturesAatish Dilip ShahAún no hay calificaciones
- Type I: Luting Agents That Include Permanent and Temporary Cements. Type II: Restorative Applications. Type III: Liner or Base ApplicationsDocumento5 páginasType I: Luting Agents That Include Permanent and Temporary Cements. Type II: Restorative Applications. Type III: Liner or Base ApplicationsSony RajbhandariAún no hay calificaciones
- Week 7 Histology Physiology of Dental Pulp MiriamDocumento4 páginasWeek 7 Histology Physiology of Dental Pulp MiriamDelaney IslipAún no hay calificaciones
- Defense Mechanism of GingivaDocumento46 páginasDefense Mechanism of GingivaSunny MaviAún no hay calificaciones
- Diagnosis and Treatment of Periodontal Disease ExplainedDocumento53 páginasDiagnosis and Treatment of Periodontal Disease ExplainedSunny MaviAún no hay calificaciones
- Diagnostic Instruments in PerioDocumento82 páginasDiagnostic Instruments in PerioSunny Mavi100% (1)
- Diagnostic Instruments in PerioDocumento82 páginasDiagnostic Instruments in PerioSunny Mavi100% (1)
- Journal of Petroleum Science and Engineering: Bin Yuan, David A. WoodDocumento13 páginasJournal of Petroleum Science and Engineering: Bin Yuan, David A. Woodarash7495Aún no hay calificaciones
- Dani RodrikDocumento12 páginasDani Rodrikprogramas4242Aún no hay calificaciones
- Emiish Me: Answer BookDocumento7 páginasEmiish Me: Answer BookNickAún no hay calificaciones
- Rubrics For Lab Report For PC1 Lab, PC2 Lab, CIC LabDocumento4 páginasRubrics For Lab Report For PC1 Lab, PC2 Lab, CIC LabHunie PopAún no hay calificaciones
- 77115 Maintenance Battery ChargerDocumento4 páginas77115 Maintenance Battery ChargerClarence ClarAún no hay calificaciones
- Application For Freshman Admission - PDF UA & PDocumento4 páginasApplication For Freshman Admission - PDF UA & PVanezza June DuranAún no hay calificaciones
- Request For Information (Rfi) : Luxury Villa at Isola Dana-09 Island - Pearl QatarDocumento1 páginaRequest For Information (Rfi) : Luxury Villa at Isola Dana-09 Island - Pearl QatarRahmat KhanAún no hay calificaciones
- Online and Payment SecurityDocumento14 páginasOnline and Payment SecurityVanezz UchihaAún no hay calificaciones
- MatrikonOPC Server For Simulation Quick Start Guide PDFDocumento2 páginasMatrikonOPC Server For Simulation Quick Start Guide PDFJorge Perez CastañedaAún no hay calificaciones
- Makerere University: Office of The Academic RegistrarDocumento2 páginasMakerere University: Office of The Academic RegistrarOPETO ISAACAún no hay calificaciones
- Cache Memory in Computer Architecture - Gate VidyalayDocumento6 páginasCache Memory in Computer Architecture - Gate VidyalayPAINAún no hay calificaciones
- 2011 REV SAE Suspension Kiszco PDFDocumento112 páginas2011 REV SAE Suspension Kiszco PDFRushik KudaleAún no hay calificaciones
- AX CLI Ref v2 4 3-20100621Documento718 páginasAX CLI Ref v2 4 3-20100621VisiGodAún no hay calificaciones
- Power Steering Rack Components and Auto Suppliers Reference GuideDocumento12 páginasPower Steering Rack Components and Auto Suppliers Reference GuideJonathan JoelAún no hay calificaciones
- Payment Solutions For Travel Platform: SabreDocumento2 páginasPayment Solutions For Travel Platform: Sabrehell nahAún no hay calificaciones
- Getting Started With DAX Formulas in Power BI, Power Pivot, and SSASDocumento19 páginasGetting Started With DAX Formulas in Power BI, Power Pivot, and SSASJohn WickAún no hay calificaciones
- Aggregate Demand and Supply: A ReviewDocumento36 páginasAggregate Demand and Supply: A ReviewYovan DharmawanAún no hay calificaciones
- 028 Ptrs Modul Matematik t4 Sel-96-99Documento4 páginas028 Ptrs Modul Matematik t4 Sel-96-99mardhiah88Aún no hay calificaciones
- MEETING OF THE BOARD OF GOVERNORS Committee on University Governance April 17, 2024Documento8 páginasMEETING OF THE BOARD OF GOVERNORS Committee on University Governance April 17, 2024Jamie BouletAún no hay calificaciones
- Computer Science Practical File WorkDocumento34 páginasComputer Science Practical File WorkArshdeep SinghAún no hay calificaciones
- Ts 391 IltDocumento5 páginasTs 391 IltFunnypoumAún no hay calificaciones
- A Survey of The Advancing Use and Development of Machine Learning in Smart ManufacturingDocumento32 páginasA Survey of The Advancing Use and Development of Machine Learning in Smart Manufacturingbeben_19Aún no hay calificaciones
- LK BMHS 30 September 2021Documento71 páginasLK BMHS 30 September 2021samudraAún no hay calificaciones
- Flex VPNDocumento3 páginasFlex VPNAnonymous nFOywQZAún no hay calificaciones
- The General Agreement On Trade in Services An IntroductionDocumento22 páginasThe General Agreement On Trade in Services An IntroductionakyregisterAún no hay calificaciones
- Virtual Content SOPDocumento11 páginasVirtual Content SOPAnezwa MpetaAún no hay calificaciones
- Activity Problem Set G4Documento5 páginasActivity Problem Set G4Cloister CapananAún no hay calificaciones