También podría gustarte
- CHAPTER 1.ppt-2Documento49 páginasCHAPTER 1.ppt-2Gemechis MergaAún no hay calificaciones
- Parasitologydrrahul 150706161018 Lva1 App6892Documento29 páginasParasitologydrrahul 150706161018 Lva1 App6892NOKHAIZ HAMMAD 2021-BS-MLS-007Aún no hay calificaciones
- Parasitology 1Documento23 páginasParasitology 1Mona AdamAún no hay calificaciones
- PARASITOLOGY NotesDocumento36 páginasPARASITOLOGY NotesTumabang DivineAún no hay calificaciones
- Introduction To Medical ParasitologyDocumento27 páginasIntroduction To Medical Parasitologyamrokhalidyousif77Aún no hay calificaciones
- 1.introduction To ParasitologyDocumento32 páginas1.introduction To ParasitologyPallavi Uday Naik100% (1)
- Parasitology: Mrs. Mehwish ZeeshanDocumento59 páginasParasitology: Mrs. Mehwish ZeeshanAlex ChagalaAún no hay calificaciones
- The Intestinal NematodesDocumento107 páginasThe Intestinal Nematodesblue_blooded23100% (1)
- Pathology, Vector Studies, and CultureDe EverandPathology, Vector Studies, and CultureJulius P. KreierCalificación: 5 de 5 estrellas5/5 (1)
- Parasitology Lec 3.01a Intestinal NematodesDocumento16 páginasParasitology Lec 3.01a Intestinal NematodesEnaWahahaAún no hay calificaciones
- Introduction To ParasitologyDocumento44 páginasIntroduction To ParasitologyRIC JOSEPH PONCIANOAún no hay calificaciones
- CestodesDocumento39 páginasCestodesNachiket Vijay PotdarAún no hay calificaciones
- TREMATODESDocumento31 páginasTREMATODESKen Mark ConcepcionAún no hay calificaciones
- Antigen and Its PropertiesDocumento20 páginasAntigen and Its Propertiestusharpremin92% (12)
- Introduction To Medical Parasitology Prepared By: Geraldine P. PulidoDocumento26 páginasIntroduction To Medical Parasitology Prepared By: Geraldine P. PulidoMark Reynie Renz SilvaAún no hay calificaciones
- Protozoans Lecture AmoebaDocumento42 páginasProtozoans Lecture Amoebablue_blooded23100% (1)
- Bachelor of Science in Medical Technology 2014Documento6 páginasBachelor of Science in Medical Technology 2014Maxine TaeyeonAún no hay calificaciones
- 1-Introduction To MicrobiologyDocumento43 páginas1-Introduction To MicrobiologyMaria AhmedAún no hay calificaciones
- NematodaDocumento96 páginasNematodaPurplesmilezAún no hay calificaciones
- Group 3 - ParasitologyDocumento8 páginasGroup 3 - Parasitologyjulo_05Aún no hay calificaciones
- Microbiology-Specimens CollectionDocumento31 páginasMicrobiology-Specimens Collectionapi-253201876100% (1)
- Clinical Parasitology LaboratoryDocumento4 páginasClinical Parasitology LaboratoryLyka ReyesAún no hay calificaciones
- Cestodes PDFDocumento171 páginasCestodes PDFsummer djAún no hay calificaciones
- Host Response To InfectionDocumento36 páginasHost Response To InfectionFrancia Toledano100% (1)
- 4-Microbiology & ParasitologyDocumento2 páginas4-Microbiology & ParasitologyIbrahimFikryAún no hay calificaciones
- TrematodesDocumento75 páginasTrematodesHann SantiagoAún no hay calificaciones
- AmoebaDocumento5 páginasAmoebasarguss14Aún no hay calificaciones
- Group 4 - General Pathology, Logic and Cytologic TechniquesDocumento11 páginasGroup 4 - General Pathology, Logic and Cytologic Techniquesjulo_05Aún no hay calificaciones
- Tissue NematodesDocumento33 páginasTissue NematodesJessiAún no hay calificaciones
- Histopathology Lecture 1 Week February 01,2020Documento44 páginasHistopathology Lecture 1 Week February 01,2020FatimaMendozaAún no hay calificaciones
- Take Home Quiz CDMDocumento3 páginasTake Home Quiz CDMapi-19786361Aún no hay calificaciones
- Cestode SDocumento38 páginasCestode SJang JangAún no hay calificaciones
- Act.1 RQ 2 Pipettes and Others 1-3Documento3 páginasAct.1 RQ 2 Pipettes and Others 1-3Francis Valdez100% (1)
- Entamoeba SPPDocumento21 páginasEntamoeba SPPragnabulletinAún no hay calificaciones
- Outline: 1. General Characteristics of Platyhelminthes 2. Classification of Platyhelminthes 3. Cestodes 4. TrematodesDocumento73 páginasOutline: 1. General Characteristics of Platyhelminthes 2. Classification of Platyhelminthes 3. Cestodes 4. TrematodesAsxe CeeAún no hay calificaciones
- Vibrio (Comma-Shaped or Curved Bacillus)Documento10 páginasVibrio (Comma-Shaped or Curved Bacillus)Ira ElizagaAún no hay calificaciones
- MICROBIODocumento158 páginasMICROBIOJoyce VillanuevaAún no hay calificaciones
- Safe Blood: Purifying the Nations Blood Supply in the Age of ADe EverandSafe Blood: Purifying the Nations Blood Supply in the Age of AAún no hay calificaciones
- Introduction To Diagnostic Parasitology: (Specimen Collection and Handling)Documento26 páginasIntroduction To Diagnostic Parasitology: (Specimen Collection and Handling)RIC JOSEPH PONCIANOAún no hay calificaciones
- Quality Assurance in BacteriologyDocumento28 páginasQuality Assurance in BacteriologyAuguz Francis Acena50% (2)
- Pathogenesis of Bacterial InfectionDocumento15 páginasPathogenesis of Bacterial InfectionMichaelJJordan100% (1)
- Questions Micro Bi LogyDocumento9 páginasQuestions Micro Bi Logymajd_hallAún no hay calificaciones
- 5-PPT For HR Used in MLSDocumento11 páginas5-PPT For HR Used in MLSNeelu MishraAún no hay calificaciones
- Pathogenesis of Bacterial Infection and Nosocomial InfectionDocumento56 páginasPathogenesis of Bacterial Infection and Nosocomial InfectionDenise Johnson0% (1)
- Chapter 05. Normal Flora of The Human BodyDocumento16 páginasChapter 05. Normal Flora of The Human BodyChino Isiah CañeteAún no hay calificaciones
- Accurate Diagnosis of Parasitic Infections Is Important To Decrease The Prevalence andDocumento4 páginasAccurate Diagnosis of Parasitic Infections Is Important To Decrease The Prevalence andManulat VicaiiAún no hay calificaciones
- Microbiology For The Health Sciences: Chapter 4. Diversity of MicroorganismsDocumento59 páginasMicrobiology For The Health Sciences: Chapter 4. Diversity of MicroorganismsHiba Abu-jumahAún no hay calificaciones
- Protozoan Maricelle ManlutacDocumento53 páginasProtozoan Maricelle ManlutacGlanela ManalotoAún no hay calificaciones
- GRAM Positive CocciDocumento67 páginasGRAM Positive CocciNoraine Princess TabangcoraAún no hay calificaciones
- Introduction To Medical ParasitologyDocumento19 páginasIntroduction To Medical ParasitologyLaila AbdulAún no hay calificaciones
- TrematodesDocumento9 páginasTrematodesLewis P. SanchezAún no hay calificaciones
- Stool AnalysisDocumento11 páginasStool AnalysisMohsen Haleem100% (1)
- Bacterial Metabolism (Eng.)Documento14 páginasBacterial Metabolism (Eng.)hengkitanjungAún no hay calificaciones
- Histology of Ear and EyeDocumento2 páginasHistology of Ear and EyeAnny Alvrz100% (1)
- 1 IntroDocumento5 páginas1 IntroJeanjayannseptoemanAún no hay calificaciones
- HISTO-S01-T01-Histology & Its Methods of StudyDocumento5 páginasHISTO-S01-T01-Histology & Its Methods of StudyShelahAún no hay calificaciones
- Tissue and Blood NematodesDocumento53 páginasTissue and Blood NematodesVincent ManganaanAún no hay calificaciones
- (Para) Introduction To Parasitology and Protozoology-Dr. Dela Rosa (Tiglao)Documento7 páginas(Para) Introduction To Parasitology and Protozoology-Dr. Dela Rosa (Tiglao)Arlene DaroAún no hay calificaciones
- Acute InflammationDocumento55 páginasAcute InflammationMohammad_Islam8790% (10)
- Para Lec 1Documento23 páginasPara Lec 1stpaulafamilyAún no hay calificaciones
- Vector ControlDocumento19 páginasVector ControlrodelagapitoAún no hay calificaciones
- Introduction To Human Resource ManagementDocumento44 páginasIntroduction To Human Resource ManagementrodelagapitoAún no hay calificaciones
- The Photographic PrinciplesDocumento32 páginasThe Photographic PrinciplesrodelagapitoAún no hay calificaciones
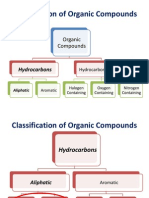
- Introduction To Organic ChemistryDocumento48 páginasIntroduction To Organic Chemistryrodelagapito100% (2)
- Blood TransfusionDocumento104 páginasBlood TransfusionrodelagapitoAún no hay calificaciones
- KolmogorovDocumento11 páginasKolmogorovrodelagapitoAún no hay calificaciones
- Principles of EpiDocumento29 páginasPrinciples of Epirodelagapito100% (1)
- SkinDocumento38 páginasSkinrodelagapito100% (1)
- Principles of Epidemiology & Epidemiologic MethodsDocumento8 páginasPrinciples of Epidemiology & Epidemiologic MethodsrodelagapitoAún no hay calificaciones
- Sinidu Final LastDocumento20 páginasSinidu Final LastAnonymous RCOlt3gAún no hay calificaciones
- Host Parasite InteractionDocumento20 páginasHost Parasite InteractionRhomizal MazaliAún no hay calificaciones
- Module 4 - Relationships in An EcosystemDocumento30 páginasModule 4 - Relationships in An EcosystemEshaaAyisha RiazAún no hay calificaciones
- Ch31 Lecture NotesDocumento6 páginasCh31 Lecture Notesrandicandi09Aún no hay calificaciones
- Bacteria and Viruses PowerPointDocumento43 páginasBacteria and Viruses PowerPointGastonMuñozAzulGmgAún no hay calificaciones
- Definitions of Parasitism Considering Its Potentially Opposing Effects at Different Levels of Hierarchical OrganizationDocumento8 páginasDefinitions of Parasitism Considering Its Potentially Opposing Effects at Different Levels of Hierarchical OrganizationwellingtonlimaAún no hay calificaciones
- Biology Today and Tomorrow With Physiology 5th Edition Starr Test Bank 1Documento26 páginasBiology Today and Tomorrow With Physiology 5th Edition Starr Test Bank 1sook100% (35)
- Module 3Documento7 páginasModule 3Rana VergaraAún no hay calificaciones
- Semi-Detailed Lesson Plan in Grade 7 I. ObjectivesDocumento7 páginasSemi-Detailed Lesson Plan in Grade 7 I. ObjectivesAngelique BarquillaAún no hay calificaciones
- Environmental Science Introduction To Environmental Science: CSPC-F-COL-13B Camarines Sur Polytechnic CollegesDocumento5 páginasEnvironmental Science Introduction To Environmental Science: CSPC-F-COL-13B Camarines Sur Polytechnic CollegesPrincess NobleAún no hay calificaciones
- Science7-Q2-Mod8 v1Documento34 páginasScience7-Q2-Mod8 v1Meryl Gallardo100% (1)
- Preferencias Alimentares de Mosquitos - EefbDocumento24 páginasPreferencias Alimentares de Mosquitos - EefbEben Leonel Albano MaiopueAún no hay calificaciones
- Predation and ParasitismDocumento23 páginasPredation and Parasitismvera febriyantiAún no hay calificaciones
- 4 Pasay S4LT Q2 W7 2Documento25 páginas4 Pasay S4LT Q2 W7 2Maria Allyza AlfajaroAún no hay calificaciones
- Biology - PiDocumento23 páginasBiology - PiTashaAún no hay calificaciones
- Gurltia Paralysans MoroniDocumento4 páginasGurltia Paralysans MoroniCristián Herrera FernándezAún no hay calificaciones
- 06 Parasitoid InsectsDocumento23 páginas06 Parasitoid InsectsvioindahAún no hay calificaciones
- The Legend of La PatasolaDocumento38 páginasThe Legend of La Patasolapaul andres rodriguez gonzalezAún no hay calificaciones
- ICAR JRF Veterinary Question Paper - PSCDocumento6 páginasICAR JRF Veterinary Question Paper - PSCSatyabrat DuttaAún no hay calificaciones
- Herd Health ManagmentDocumento10 páginasHerd Health ManagmentAjasrAún no hay calificaciones
- Palmones Parasitology Lab TransesDocumento19 páginasPalmones Parasitology Lab TransesJISOO KimAún no hay calificaciones
- EoLS - Poinar (2007) NematodaDocumento4 páginasEoLS - Poinar (2007) NematodaNICOLAS BORJA MARTINEZAún no hay calificaciones
- طفيليات عملي الحكمة المعمل 1Documento5 páginasطفيليات عملي الحكمة المعمل 1Mohammed AbdullahAún no hay calificaciones
- Bronstispa LonggisimaDocumento103 páginasBronstispa LonggisimaPca ZdnAún no hay calificaciones
- Introduction To ParasitologyDocumento21 páginasIntroduction To Parasitologyning ningAún no hay calificaciones
- Biological InteractionDocumento17 páginasBiological InteractionArchana SharmaAún no hay calificaciones
- Reading - Cas - Text Structure and PurposeDocumento5 páginasReading - Cas - Text Structure and PurposePhương Linh LêAún no hay calificaciones
- Trypanosoma GambienesDocumento5 páginasTrypanosoma Gambienesapi-481318101Aún no hay calificaciones
- Bronstein 1994Documento4 páginasBronstein 1994FATIMA MARIAN GARRIDO VARGASAún no hay calificaciones
- MicrobiologyDocumento108 páginasMicrobiologyHampson Malekano100% (1)