También podría gustarte
- Case Write-Up 1Documento16 páginasCase Write-Up 1Zharif Fikri100% (3)
- Morning Report: Jawaria K. Alam, MD/PGY3Documento20 páginasMorning Report: Jawaria K. Alam, MD/PGY3Emily EresumaAún no hay calificaciones
- Imed Case 5Documento11 páginasImed Case 5Shakshi RainaAún no hay calificaciones
- Problem Based LearningDocumento2 páginasProblem Based LearningKate XuAún no hay calificaciones
- First Half Heme Onc Bae PresentationDocumento22 páginasFirst Half Heme Onc Bae PresentationanthonyAún no hay calificaciones
- These Are Hospital PresentationsDocumento73 páginasThese Are Hospital PresentationsMahmoud AjinehAún no hay calificaciones
- Acute Appendicitis 3Documento8 páginasAcute Appendicitis 3Aiman ArifinAún no hay calificaciones
- AscitesDocumento50 páginasAscitesDiponkar PoddarAún no hay calificaciones
- 2b Case StudyDocumento5 páginas2b Case StudyCkaye MontilAún no hay calificaciones
- AnasarcaDocumento54 páginasAnasarcaSulaiman TahsinAún no hay calificaciones
- Apriyanto Lifandy Desmy FadillahDocumento38 páginasApriyanto Lifandy Desmy FadillahdesmyyAún no hay calificaciones
- CKDDocumento48 páginasCKDJuniorAún no hay calificaciones
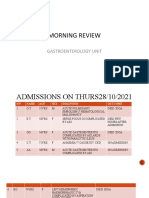
- MR GastroDocumento31 páginasMR GastroAdefuye AbiolaAún no hay calificaciones
- Sample Case 1Documento4 páginasSample Case 1AngelaTrinidadAún no hay calificaciones
- Endocrinology Clinical History: Extremity Weakness Case HistoryDocumento2 páginasEndocrinology Clinical History: Extremity Weakness Case HistoryramkodAún no hay calificaciones
- Acute Chronic PancreatitisDocumento38 páginasAcute Chronic PancreatitisAliyah Tofani PawelloiAún no hay calificaciones
- Git MCQ Valume ADocumento37 páginasGit MCQ Valume AAhmed ElwassiefAún no hay calificaciones
- Sickle CellDocumento47 páginasSickle CellEmily EresumaAún no hay calificaciones
- CA Pancreas BasirDocumento9 páginasCA Pancreas BasirwhosenahAún no hay calificaciones
- Identification DataDocumento15 páginasIdentification DataFariezuan HamidAún no hay calificaciones
- A 20-Year-Old Female With Bloody DiarrhoeaDocumento41 páginasA 20-Year-Old Female With Bloody DiarrhoeaMatthew LoopAún no hay calificaciones
- Case Study:: Breathe ShortnessDocumento6 páginasCase Study:: Breathe ShortnessAsifa SafdarAún no hay calificaciones
- Case PresentationDocumento31 páginasCase PresentationArsalan NadeemAún no hay calificaciones
- Emphysematous Pyelonephritis: Joint Urology ConferenceDocumento32 páginasEmphysematous Pyelonephritis: Joint Urology ConferencecosmicdaeAún no hay calificaciones
- Duty Report Er 23 07 2015Documento25 páginasDuty Report Er 23 07 2015Auditya WidyasariAún no hay calificaciones
- Acute and Chronic HepatitisDocumento72 páginasAcute and Chronic HepatitisArun George100% (3)
- Dr. Farin's Grand Round Presentation 31.09.23Documento75 páginasDr. Farin's Grand Round Presentation 31.09.23Anika TasnimAún no hay calificaciones
- Hemolytic Uremic Syndrome 8.13.18Documento34 páginasHemolytic Uremic Syndrome 8.13.18Emily EresumaAún no hay calificaciones
- CFGVDocumento28 páginasCFGVmyolie wuAún no hay calificaciones
- Name: Wong Wai Kheong Matrix No: BMS12081154Documento13 páginasName: Wong Wai Kheong Matrix No: BMS12081154myolie wuAún no hay calificaciones
- Nusing Assessment Guide: Kidney Failure (CKD) Area: CCUDocumento15 páginasNusing Assessment Guide: Kidney Failure (CKD) Area: CCUAbbas AwfiAún no hay calificaciones
- Nusing Assessment Guide: Kidney Failure (CKD) Area: CCUDocumento15 páginasNusing Assessment Guide: Kidney Failure (CKD) Area: CCUAbbas AwfiAún no hay calificaciones
- Diarrhea 2Documento27 páginasDiarrhea 2nityaprasanta4679Aún no hay calificaciones
- Sirosis HepatisDocumento29 páginasSirosis HepatisXaverius da CunhaAún no hay calificaciones
- Acute Appendicitis: Surgical PostingDocumento8 páginasAcute Appendicitis: Surgical PostingGraldoAún no hay calificaciones
- Cannabinoid Hyperemesis SyndromeDocumento24 páginasCannabinoid Hyperemesis SyndromeEmily EresumaAún no hay calificaciones
- Morning Report 9/5/18: Adam Cardullo, MD Pgy - 2Documento22 páginasMorning Report 9/5/18: Adam Cardullo, MD Pgy - 2Emily EresumaAún no hay calificaciones
- Case Presentation Complicated Crohn'sDocumento23 páginasCase Presentation Complicated Crohn'sRamy ElbarodyAún no hay calificaciones
- Case Report Gastric PerforationDocumento58 páginasCase Report Gastric PerforationAlwin RaisAún no hay calificaciones
- Unstable Angina With Underlying DyslipidaemiaDocumento9 páginasUnstable Angina With Underlying DyslipidaemiaAiman ArifinAún no hay calificaciones
- Hematology CasesDocumento10 páginasHematology Casesuyes100% (1)
- YL3 GI End of Module Activity Complex Task - StudentsDocumento1 páginaYL3 GI End of Module Activity Complex Task - StudentsAnonymous Xlpj86laAún no hay calificaciones
- Accident and Emergency Posting Case Write UpDocumento8 páginasAccident and Emergency Posting Case Write UpAmbhi Gana0% (1)
- Case Report On Hepatitis/Cirrhosis: Presented By: Basnet, PragyanDocumento41 páginasCase Report On Hepatitis/Cirrhosis: Presented By: Basnet, PragyanBasneyatPragyanAún no hay calificaciones
- Liver Cirrhosis: DR - Aryadevi A SDocumento89 páginasLiver Cirrhosis: DR - Aryadevi A SMahesh PethkarAún no hay calificaciones
- Case Presentation: East Avenue Medical Center Female Surgical Ward Group DDocumento32 páginasCase Presentation: East Avenue Medical Center Female Surgical Ward Group DKyle TampoyaAún no hay calificaciones
- HPB DiseaseDocumento35 páginasHPB Diseaseapi-195799092Aún no hay calificaciones
- Acute Liver FailureDocumento57 páginasAcute Liver FailureashokgswaminathanAún no hay calificaciones
- Abnormal LTs 2014Documento63 páginasAbnormal LTs 2014Robert G. Gish, MDAún no hay calificaciones
- Diabetes Mellitus Complte LONG 2Documento56 páginasDiabetes Mellitus Complte LONG 2John Vincent Dy OcampoAún no hay calificaciones
- Cwu SurgeryDocumento16 páginasCwu SurgeryAslah NabilahAún no hay calificaciones
- NC Rara HemaDocumento18 páginasNC Rara HemaDodi DiAún no hay calificaciones
- Git MCQ Valume BDocumento28 páginasGit MCQ Valume BAhmed ElwassiefAún no hay calificaciones
- A) Importance of The Case StudyDocumento73 páginasA) Importance of The Case StudyRaidis PangilinanAún no hay calificaciones
- Acute Appendicitis 2Documento7 páginasAcute Appendicitis 2Aiman ArifinAún no hay calificaciones
- Case Study On BronchitisDocumento19 páginasCase Study On BronchitisSuchitaAún no hay calificaciones
- Gastrointestinal System Review PPT 2022 (Autosaved)Documento30 páginasGastrointestinal System Review PPT 2022 (Autosaved)LalaAún no hay calificaciones
- Fever of Unknown Origin (FUO)Documento55 páginasFever of Unknown Origin (FUO)mohamed hanyAún no hay calificaciones
- Petersen Ucsd PHS, Eis 5-25-2010 97Documento53 páginasPetersen Ucsd PHS, Eis 5-25-2010 97grahamabra100% (1)
- Fifteen Campus Map 2009Documento1 páginaFifteen Campus Map 2009grahamabraAún no hay calificaciones
- Review Small Bowel Colon: of The ANDDocumento43 páginasReview Small Bowel Colon: of The ANDgrahamabraAún no hay calificaciones
- Renal Survival GuideDocumento5 páginasRenal Survival GuidegrahamabraAún no hay calificaciones
- ABIM Logy Review 2010Documento111 páginasABIM Logy Review 2010grahamabraAún no hay calificaciones
- Evidence Based MedicineDocumento10 páginasEvidence Based MedicinegrahamabraAún no hay calificaciones
- CME JRK Brochure 2010 (10-22)Documento6 páginasCME JRK Brochure 2010 (10-22)grahamabraAún no hay calificaciones
- Internal Medicine Board ReviewDocumento64 páginasInternal Medicine Board Reviewgrahamabra50% (2)
- 2010 Allergy and Immunology Board ReviewDocumento132 páginas2010 Allergy and Immunology Board Reviewgrahamabra50% (2)
- Carriage RequirementsDocumento63 páginasCarriage RequirementsFred GrosfilerAún no hay calificaciones
- Heterogeneity in Macroeconomics: Macroeconomic Theory II (ECO-504) - Spring 2018Documento5 páginasHeterogeneity in Macroeconomics: Macroeconomic Theory II (ECO-504) - Spring 2018Gabriel RoblesAún no hay calificaciones
- Turn Around Coordinator Job DescriptionDocumento2 páginasTurn Around Coordinator Job DescriptionMikeAún no hay calificaciones
- Arens - Auditing and Assurance Services 15e-2Documento17 páginasArens - Auditing and Assurance Services 15e-2Magdaline ChuaAún no hay calificaciones
- MASONRYDocumento8 páginasMASONRYJowelyn MaderalAún no hay calificaciones
- The Person Environment Occupation (PEO) Model of Occupational TherapyDocumento15 páginasThe Person Environment Occupation (PEO) Model of Occupational TherapyAlice GiffordAún no hay calificaciones
- Carob-Tree As CO2 Sink in The Carbon MarketDocumento5 páginasCarob-Tree As CO2 Sink in The Carbon MarketFayssal KartobiAún no hay calificaciones
- SSGC-RSGLEG Draft Study On The Applicability of IAL To Cyber Threats Against Civil AviationDocumento41 páginasSSGC-RSGLEG Draft Study On The Applicability of IAL To Cyber Threats Against Civil AviationPrachita AgrawalAún no hay calificaciones
- Köppen Climate Classification - Wikipedia, The Free EncyclopediaDocumento15 páginasKöppen Climate Classification - Wikipedia, The Free EncyclopediaAndreea Tataru StanciAún no hay calificaciones
- Aleksandrov I Dis 1-50.ru - enDocumento50 páginasAleksandrov I Dis 1-50.ru - enNabeel AdilAún no hay calificaciones
- Benevisión N15 Mindray Service ManualDocumento123 páginasBenevisión N15 Mindray Service ManualSulay Avila LlanosAún no hay calificaciones
- Ozone Therapy - A Clinical Review A. M. Elvis and J. S. EktaDocumento5 páginasOzone Therapy - A Clinical Review A. M. Elvis and J. S. Ektatahuti696Aún no hay calificaciones
- Parliament of India: Rajya SabhaDocumento64 páginasParliament of India: Rajya SabhaSivapothuraju KonathalaAún no hay calificaciones
- Application of Graph Theory in Operations ResearchDocumento3 páginasApplication of Graph Theory in Operations ResearchInternational Journal of Innovative Science and Research Technology100% (2)
- Richardson Heidegger PDFDocumento18 páginasRichardson Heidegger PDFweltfremdheitAún no hay calificaciones
- IKEA SHANGHAI Case StudyDocumento5 páginasIKEA SHANGHAI Case StudyXimo NetteAún no hay calificaciones
- DarcDocumento9 páginasDarcJunior BermudezAún no hay calificaciones
- The Doshas in A Nutshell - : Vata Pitta KaphaDocumento1 páginaThe Doshas in A Nutshell - : Vata Pitta KaphaCheryl LynnAún no hay calificaciones
- Lesson 5 Designing and Developing Social AdvocacyDocumento27 páginasLesson 5 Designing and Developing Social Advocacydaniel loberizAún no hay calificaciones
- ISO 9001 2015 AwarenessDocumento23 páginasISO 9001 2015 AwarenessSeni Oke0% (1)
- II 2022 06 Baena-Rojas CanoDocumento11 páginasII 2022 06 Baena-Rojas CanoSebastian GaonaAún no hay calificaciones
- GT-N7100-Full Schematic PDFDocumento67 páginasGT-N7100-Full Schematic PDFprncha86% (7)
- Oracle - Prep4sure.1z0 068.v2016!07!12.by - Lana.60qDocumento49 páginasOracle - Prep4sure.1z0 068.v2016!07!12.by - Lana.60qLuis AlfredoAún no hay calificaciones
- Equivalent Fractions Activity PlanDocumento6 páginasEquivalent Fractions Activity Planapi-439333272Aún no hay calificaciones
- Specificities of The Terminology in AfricaDocumento2 páginasSpecificities of The Terminology in Africapaddy100% (1)
- Origami Oso HormigueroDocumento9 páginasOrigami Oso HormigueroRogelio CerdaAún no hay calificaciones
- Chapter 1 ClassnotesDocumento35 páginasChapter 1 ClassnotesAllison CasoAún no hay calificaciones
- 2009 2011 DS Manual - Club Car (001-061)Documento61 páginas2009 2011 DS Manual - Club Car (001-061)misaAún no hay calificaciones
- Post Appraisal InterviewDocumento3 páginasPost Appraisal InterviewNidhi D100% (1)
- 1.technical Specifications (Piling)Documento15 páginas1.technical Specifications (Piling)Kunal Panchal100% (2)