También podría gustarte
- Anestesi Pada OrtopediDocumento20 páginasAnestesi Pada OrtopediLeo Kolong100% (1)
- Persiapan Anestesi UmumDocumento12 páginasPersiapan Anestesi UmumNadya Fairida33% (3)
- Manajemen Anestesi Pada Bedah DaruratDocumento22 páginasManajemen Anestesi Pada Bedah Daruratneenan100% (1)
- Ambulatory AnesthesiaDocumento16 páginasAmbulatory Anesthesiad_learnAún no hay calificaciones
- Mengakses Jalan Nafas Dengan Metode Lemon ScoreDocumento41 páginasMengakses Jalan Nafas Dengan Metode Lemon ScoreAnonymous N0FpVJ0d50% (2)
- LMADocumento20 páginasLMATirta SaputraAún no hay calificaciones
- OLV-Double Lumen TubeDocumento12 páginasOLV-Double Lumen TubeMuhammad Ridho AdityaAún no hay calificaciones
- Obat-Obatan Anestesi PDFDocumento26 páginasObat-Obatan Anestesi PDFEka Sulistyowati P50% (2)
- Target Controled InfusionDocumento36 páginasTarget Controled Infusionvictor0% (1)
- Saddle Block AnestesiDocumento19 páginasSaddle Block AnestesiAndi PakdheeAún no hay calificaciones
- Anestesi Umum Dan RegionalDocumento78 páginasAnestesi Umum Dan RegionalBagusIrawanWahidilmanAún no hay calificaciones
- LAPORAN KASUS OBSTRUKSI BILIERDocumento18 páginasLAPORAN KASUS OBSTRUKSI BILIERnadyajondri50% (2)
- Anestesi Pada Bedah Rawat JalanDocumento22 páginasAnestesi Pada Bedah Rawat JalanAnestesi StaticsAún no hay calificaciones
- Anestesi dan pengaruh merokokDocumento6 páginasAnestesi dan pengaruh merokokrobbyalfadliAún no hay calificaciones
- ANESTESI PADA PASIEN ARITMIADocumento32 páginasANESTESI PADA PASIEN ARITMIARichesio Sapata TomokumoroAún no hay calificaciones
- Bone Cement Implantation SyndromeDocumento3 páginasBone Cement Implantation SyndromeIqbal HarzikyAún no hay calificaciones
- Presentasi EkstubasiDocumento9 páginasPresentasi EkstubasiPmk UntanAún no hay calificaciones
- Lapkas Anastesi Umum Pada Eklampsia Dan HELLP SyndromeDocumento44 páginasLapkas Anastesi Umum Pada Eklampsia Dan HELLP SyndromeAngelinAún no hay calificaciones
- ANESTESIDocumento9 páginasANESTESIDewangga LeonitaAún no hay calificaciones
- Referat FentanylDocumento28 páginasReferat FentanylhengkiAún no hay calificaciones
- Anestesi Untuk Pasien Luka BakarDocumento7 páginasAnestesi Untuk Pasien Luka BakarVictorJansenAún no hay calificaciones
- Efek Anestesi Inhalasi Terhadap Sistem PernafasanDocumento39 páginasEfek Anestesi Inhalasi Terhadap Sistem PernafasanRavenAún no hay calificaciones
- Train of Four R1Documento7 páginasTrain of Four R1Rafael BagusAún no hay calificaciones
- Managemen Anestesi Pada Pasien Efusi PleuraDocumento16 páginasManagemen Anestesi Pada Pasien Efusi Pleurabra56juhAún no hay calificaciones
- EKSTUBASIDocumento20 páginasEKSTUBASIRomi Mauliza FauziAún no hay calificaciones
- Inhalasi SistemDocumento4 páginasInhalasi SistemDavid MudlofieAún no hay calificaciones
- Anestesia TorakotomiDocumento37 páginasAnestesia TorakotomiabdulAún no hay calificaciones
- NYERI KEPALADocumento3 páginasNYERI KEPALAHameldo Andika PattinasaranyAún no hay calificaciones
- Manajemen Bronkospasme Durante General Anastesi Mas RezaDocumento14 páginasManajemen Bronkospasme Durante General Anastesi Mas RezaAldy BimaAún no hay calificaciones
- Hormon TiroidDocumento33 páginasHormon TiroidJulius SantosoAún no hay calificaciones
- Anestesi UmumDocumento42 páginasAnestesi UmumCecilia Casandra UneputtyAún no hay calificaciones
- Terapi Cairan AnestesiDocumento13 páginasTerapi Cairan AnestesiDeri Arara67% (3)
- ANESTESI AAA RUPTURDocumento7 páginasANESTESI AAA RUPTURFakhri Nade100% (1)
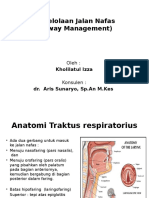
- Pengelolaan Jalan NafasDocumento25 páginasPengelolaan Jalan NafaskholilaizzaAún no hay calificaciones
- Caudal AnestesiDocumento16 páginasCaudal AnestesiSyandri Agus RizkyAún no hay calificaciones
- Obat Pelumpuh OtotDocumento28 páginasObat Pelumpuh OtotSamuel G H SimbolonAún no hay calificaciones
- Referat Triage AnestesiDocumento8 páginasReferat Triage AnestesidayungAún no hay calificaciones
- Anestesi - Managemen Ventilator Pada Anestesi UmumDocumento18 páginasAnestesi - Managemen Ventilator Pada Anestesi UmumDameria Purba0% (1)
- TIVA KURETASEDocumento30 páginasTIVA KURETASELestariNurIndrianiAún no hay calificaciones
- Tri RefaratDocumento20 páginasTri RefaratTri Wahyuni ApriantiAún no hay calificaciones
- Pre-renal Acute Renal FailureDocumento36 páginasPre-renal Acute Renal FailurezeniahudaAún no hay calificaciones
- Awake IntubationDocumento13 páginasAwake IntubationYunitaIrhamAún no hay calificaciones
- Case AnestesiDocumento23 páginasCase AnestesiChristianMelkaAún no hay calificaciones
- LAPORAN PELATIHAN PERAWAT TERAMPIL ANESTESI ANGKATAN 17Documento33 páginasLAPORAN PELATIHAN PERAWAT TERAMPIL ANESTESI ANGKATAN 17Novi KartikadewiAún no hay calificaciones
- Total Spinal AnesthesiaDocumento14 páginasTotal Spinal AnesthesiaAnonymous 2kPiJhIlFAún no hay calificaciones
- Epidural AnestesiDocumento17 páginasEpidural AnestesiNur Alty FitriantiAún no hay calificaciones
- CBT Agustus 2018Documento61 páginasCBT Agustus 2018DendyAún no hay calificaciones
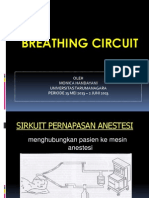
- Sirkuit AnestesiDocumento24 páginasSirkuit AnestesiAurelia SuryaniAún no hay calificaciones
- Bab 38 Anestesi Untuk Bedah OrthopediDocumento25 páginasBab 38 Anestesi Untuk Bedah OrthopedisiskaAún no hay calificaciones
- Resusitasi CairanDocumento39 páginasResusitasi CairanhpyozaAún no hay calificaciones
- Analegesik Multimodal Untuk Pengelolaan Nyeri Pasca OperasiDocumento44 páginasAnalegesik Multimodal Untuk Pengelolaan Nyeri Pasca Operasigw_liaAún no hay calificaciones
- Alat Dan Mesin AnestesiDocumento40 páginasAlat Dan Mesin AnestesiYusufHarpanAún no hay calificaciones
- DOSIS OBAT ANESTESIDocumento4 páginasDOSIS OBAT ANESTESIMakhury MilanistiAún no hay calificaciones
- Mesin AnestesiaDocumento16 páginasMesin AnestesiaAlif Putri YustikaAún no hay calificaciones
- Anestesi Pada Laparaskopi CholesistektomiDocumento6 páginasAnestesi Pada Laparaskopi CholesistektomiBayu Residewanto PutroAún no hay calificaciones
- Mendelson SyndromeDocumento12 páginasMendelson SyndromeIkhsan AmadeaAún no hay calificaciones
- ANESTESI UMUM Dan REGIONALDocumento77 páginasANESTESI UMUM Dan REGIONALhennyoktaAún no hay calificaciones
- KOMPLIKASI ANESTESIADocumento39 páginasKOMPLIKASI ANESTESIATopan Aditya HandokoAún no hay calificaciones
- CSS Aldo Victoria Komplikasi Anestesi Post OperasiDocumento26 páginasCSS Aldo Victoria Komplikasi Anestesi Post OperasiGemantri veyonda ZikryAún no hay calificaciones
- Anestesi Umum Pada KraniotomiDocumento37 páginasAnestesi Umum Pada Kraniotomimeitria nur sabrinaAún no hay calificaciones
- MI 4 - Tatalaksana Gizi Buruk Pada Balita Di Layanan Rawat JalanDocumento50 páginasMI 4 - Tatalaksana Gizi Buruk Pada Balita Di Layanan Rawat JalanDwi Cahayani UtamiAún no hay calificaciones
- Resep MancaDocumento10 páginasResep MancaArik BlizAún no hay calificaciones
- 1.1.1.1 SK Jenis Pelayanan Yang Disediakan Puskesmas-1Documento4 páginas1.1.1.1 SK Jenis Pelayanan Yang Disediakan Puskesmas-1Dwi Cahayani UtamiAún no hay calificaciones
- 1.1.1.1 SK Jenis Pelayanan Yang Disediakan Puskesmas-1Documento4 páginas1.1.1.1 SK Jenis Pelayanan Yang Disediakan Puskesmas-1Dwi Cahayani UtamiAún no hay calificaciones
- 1 Pengantar Audit Medik Baru (Hanevi Djasri)Documento20 páginas1 Pengantar Audit Medik Baru (Hanevi Djasri)Bella Afrian DientaniAún no hay calificaciones
- Asesment PasienDocumento52 páginasAsesment PasienDwi Cahayani UtamiAún no hay calificaciones
- Belajar Nahwu Dari NolDocumento5 páginasBelajar Nahwu Dari NolAbu Royan100% (1)
- Inkontinensia Urin Pada AnakDocumento7 páginasInkontinensia Urin Pada AnakSalilah MahfudzAún no hay calificaciones
- 1 Alrm Hiv 30 SlideDocumento30 páginas1 Alrm Hiv 30 SlideDizi BellAún no hay calificaciones
- Sop Menjalin Komunikasi Dengan Masyarakat-1Documento2 páginasSop Menjalin Komunikasi Dengan Masyarakat-1Dwi Cahayani UtamiAún no hay calificaciones
- 1.1.1.1 SK Jenis Pelayanan Yang Disediakan Puskesmas-1Documento4 páginas1.1.1.1 SK Jenis Pelayanan Yang Disediakan Puskesmas-1Dwi Cahayani UtamiAún no hay calificaciones
- Sop Menjalin Komunikasi Dengan Masyarakat-1Documento2 páginasSop Menjalin Komunikasi Dengan Masyarakat-1Dwi Cahayani UtamiAún no hay calificaciones
- Revisi HepatitisDocumento10 páginasRevisi HepatitisDwi Cahayani UtamiAún no hay calificaciones
- 06 BAB IV Rencana Strategis BisnisDocumento45 páginas06 BAB IV Rencana Strategis BisnisDwi Cahayani UtamiAún no hay calificaciones
- Indonesia Bebas RokokDocumento2 páginasIndonesia Bebas RokokDwi Cahayani UtamiAún no hay calificaciones
- Berita Acara PelaksanaanDocumento1 páginaBerita Acara PelaksanaanDwi Cahayani UtamiAún no hay calificaciones
- Essay ElfaDocumento1 páginaEssay ElfaDwi Cahayani UtamiAún no hay calificaciones
- AsslmlkmDocumento3 páginasAsslmlkmDwi Cahayani UtamiAún no hay calificaciones
- Bab IiDocumento20 páginasBab IiDwi Cahayani UtamiAún no hay calificaciones
- Korteks Ginjal Normal Yaitu Homogen Dan Hypoechoic Ke Hati Dan LimpaDocumento2 páginasKorteks Ginjal Normal Yaitu Homogen Dan Hypoechoic Ke Hati Dan LimpaDwi Cahayani UtamiAún no hay calificaciones
- Abdomen Akut ModifikasiDocumento27 páginasAbdomen Akut ModifikasiDwi Cahayani UtamiAún no hay calificaciones
- Korteks Ginjal Normal Yaitu Homogen Dan Hypoechoic Ke Hati Dan LimpaDocumento2 páginasKorteks Ginjal Normal Yaitu Homogen Dan Hypoechoic Ke Hati Dan LimpaDwi Cahayani UtamiAún no hay calificaciones
- Growth Hormone Atau Hormon PertumbuhanDocumento2 páginasGrowth Hormone Atau Hormon PertumbuhanDwi Cahayani UtamiAún no hay calificaciones
- Cover Tinjauan PustakaDocumento1 páginaCover Tinjauan PustakaDwi Cahayani UtamiAún no hay calificaciones
- Sindrom NefrotikDocumento12 páginasSindrom NefrotikDwi Cahayani UtamiAún no hay calificaciones
- Meningitis PDFDocumento8 páginasMeningitis PDFMeriana Puspita AtmajaAún no hay calificaciones
- Komplikasi Journal ReadingDocumento3 páginasKomplikasi Journal ReadingDwi Cahayani UtamiAún no hay calificaciones
- Kasus 3 Dr. YasmarDocumento8 páginasKasus 3 Dr. YasmarDwi Cahayani UtamiAún no hay calificaciones
- Teh ChandraDocumento1 páginaTeh ChandraDwi Cahayani UtamiAún no hay calificaciones
- Perseptoran Sindroma NefrotikDocumento17 páginasPerseptoran Sindroma NefrotikDwi Cahayani UtamiAún no hay calificaciones