También podría gustarte
- BoneDocumento68 páginasBonedr_asaleh100% (2)
- Mark Klimek Blue BookDocumento200 páginasMark Klimek Blue BookOyebamiji Emmanuel96% (25)
- Infertility - Definition, Causes, Diagnostic Procedures AND CouncellingDocumento37 páginasInfertility - Definition, Causes, Diagnostic Procedures AND CouncellingvincentsharonAún no hay calificaciones
- Physiology of MenstruationDocumento52 páginasPhysiology of Menstruationmahirad001100% (2)
- NeckDocumento67 páginasNeckdr_asaleh100% (1)
- Ovarian and Uterine Cycle - My PDocumento23 páginasOvarian and Uterine Cycle - My PAzifah Zakaria100% (2)
- MATERNAL AND CHILD HEALTH NURSINGDocumento40 páginasMATERNAL AND CHILD HEALTH NURSINGTina Talmadge100% (5)
- Excel Revise Human Biology in a MonthDocumento30 páginasExcel Revise Human Biology in a Monthdanlayton100% (4)
- Maternal and Child Health NursingDocumento22 páginasMaternal and Child Health NursingRam Van MunsterAún no hay calificaciones
- Evaluation of The Infertility CoupleDocumento19 páginasEvaluation of The Infertility Coupleapi-3705046Aún no hay calificaciones
- Paediatric OrthopaedicDocumento77 páginasPaediatric Orthopaedicdr_asalehAún no hay calificaciones
- Maternal and Child Health NursingDocumento39 páginasMaternal and Child Health NursingRena VilAún no hay calificaciones
- Yoni Steam Treatment: Book Your AppointmentDocumento2 páginasYoni Steam Treatment: Book Your AppointmentGopal Kaushik100% (1)
- MATERNAL AND CHILD HEALTH NURSINGDocumento40 páginasMATERNAL AND CHILD HEALTH NURSINGArlyn Faith AlvarezAún no hay calificaciones
- Menstruatio N: Prepared By: Lirio, Riza D. BSN 2-1Documento26 páginasMenstruatio N: Prepared By: Lirio, Riza D. BSN 2-1Eidyc_Etak_Sin_8542Aún no hay calificaciones
- Reproductive SystemDocumento35 páginasReproductive SystemSYDNIKA AIRA CARBONILLAAún no hay calificaciones
- Menstrual Disorder and Abnormal BleedingDocumento9 páginasMenstrual Disorder and Abnormal Bleedingdr_asalehAún no hay calificaciones
- Endocrinology NotesDocumento24 páginasEndocrinology NotesEmily Dong100% (1)
- Breast LumpDocumento26 páginasBreast Lumpdr_asaleh100% (2)
- MCHN Reviewer 1Documento24 páginasMCHN Reviewer 1Steam LcAún no hay calificaciones
- Summative Test Reviews in ScienceDocumento19 páginasSummative Test Reviews in ScienceZyra Jean Castañeda Canseco100% (1)
- Notes-Maternal Health NursingDocumento22 páginasNotes-Maternal Health NursingRachael Crossgrove100% (4)
- Puberty and Reproductive SystemDocumento17 páginasPuberty and Reproductive SystemEndlesly Amor DionisioAún no hay calificaciones
- Urinary IncontinenceDocumento66 páginasUrinary Incontinencedr_asaleh100% (1)
- Biochemical Methods ObgDocumento25 páginasBiochemical Methods ObgRupali AroraAún no hay calificaciones
- A Round Ligaments: 1. Which Structure Provides The Major Support To The Uterus and Cervix?Documento10 páginasA Round Ligaments: 1. Which Structure Provides The Major Support To The Uterus and Cervix?Nikhil Tyagi100% (1)
- OB - Answer KeyDocumento10 páginasOB - Answer KeyAshley Ann Flores100% (1)
- Gender and Society - Modules 2 & 3Documento17 páginasGender and Society - Modules 2 & 3Lexter JonAún no hay calificaciones
- Uterine FibroidsDocumento25 páginasUterine FibroidsMarie Eulie PatinoAún no hay calificaciones
- Maternal and Child Health NursingDocumento15 páginasMaternal and Child Health NursingJoshua VillarbaAún no hay calificaciones
- Physiological Changes in PregnancyDocumento35 páginasPhysiological Changes in PregnancyRocio SandersAún no hay calificaciones
- Maternal Health Nursing - 50 Item Without RatioDocumento3 páginasMaternal Health Nursing - 50 Item Without RatioDennis Nabor Muñoz, RN,RMAún no hay calificaciones
- Ovulation and Conception - Normal PregnancyDocumento8 páginasOvulation and Conception - Normal Pregnancyapi-3705046Aún no hay calificaciones
- Female Sub FertilityDocumento75 páginasFemale Sub FertilityIshaThapaAún no hay calificaciones
- Ovulation Pcos OhssDocumento68 páginasOvulation Pcos OhssPrakash DhungelAún no hay calificaciones
- Maternal and Child Health Nursing: Menstruation, Fertilization, and ImplantationDocumento45 páginasMaternal and Child Health Nursing: Menstruation, Fertilization, and ImplantationKaye OrtegaAún no hay calificaciones
- (Text) Maternal and Child Health NursingDocumento40 páginas(Text) Maternal and Child Health NursingVia H.Aún no hay calificaciones
- Dasar2 Biomolekuler Repro WanitaDocumento51 páginasDasar2 Biomolekuler Repro WanitaFitriaAún no hay calificaciones
- Vaginal Bleeding During PregnancyDocumento67 páginasVaginal Bleeding During PregnancyLunaLureAún no hay calificaciones
- Diagnosis of Pregnancy - SamyaDocumento58 páginasDiagnosis of Pregnancy - Samyaragulraj6699Aún no hay calificaciones
- 1 - Physiology of The Menstrual CycleDocumento17 páginas1 - Physiology of The Menstrual CycleMalak Ahmed 2295Aún no hay calificaciones
- Clinical Activities: A. Pre - ConsultationDocumento13 páginasClinical Activities: A. Pre - ConsultationerykafadsAún no hay calificaciones
- Reproductive System: Dr. Dicky Moch. Rizal, Mkes, Spand Bag. Ilmu Faal, FK UgmDocumento94 páginasReproductive System: Dr. Dicky Moch. Rizal, Mkes, Spand Bag. Ilmu Faal, FK UgmNi Made Dwiki AndriyaniAún no hay calificaciones
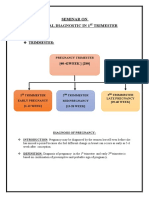
- Maternal Diagnostic in 1ST Trimester 2022Documento15 páginasMaternal Diagnostic in 1ST Trimester 2022Manoj DongarwarAún no hay calificaciones
- Kuliah PK2 TESKehamilanJULI2010Documento38 páginasKuliah PK2 TESKehamilanJULI2010Fetty NataliaAún no hay calificaciones
- Fertility and SubfertilityDocumento95 páginasFertility and SubfertilitydidiAún no hay calificaciones
- Diagnostic ApprDocumento33 páginasDiagnostic ApprNicole ArandingAún no hay calificaciones
- Understanding the Ovarian CycleDocumento52 páginasUnderstanding the Ovarian CycleLei Jenevive UmbayAún no hay calificaciones
- 5.menstrual CycleDocumento62 páginas5.menstrual CycleQaiser InayatAún no hay calificaciones
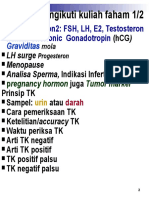
- Graviditas: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic GonadotropinDocumento32 páginasGraviditas: Faham Hormon2: FSH, LH, E2, Testosteron Human Chorionic Gonadotropinruth thauladanAún no hay calificaciones
- 68 Abnormal PeuperiumDocumento44 páginas68 Abnormal PeuperiumGodsonYeboah-AwudziAún no hay calificaciones
- Good Afternoon: Prepared byDocumento102 páginasGood Afternoon: Prepared byKrishna PatelAún no hay calificaciones
- I. Anatomy & Physiology: Readiness For Child BearingDocumento3 páginasI. Anatomy & Physiology: Readiness For Child BearingRalph Tama Mangacop BenitoAún no hay calificaciones
- Female Reproductive Hormones and the Menstrual CycleDocumento32 páginasFemale Reproductive Hormones and the Menstrual Cycleruth thauladanAún no hay calificaciones
- Angrej Sir Obstetrics NotesssDocumento119 páginasAngrej Sir Obstetrics Notessslakhwinder batthAún no hay calificaciones
- MK Disorders of Menstruation (OBGY)Documento76 páginasMK Disorders of Menstruation (OBGY)Moses Jr KazevuAún no hay calificaciones
- Project - : Menstrual CycleDocumento20 páginasProject - : Menstrual CycleJIBAN KUMAR DASAún no hay calificaciones
- Physiology of Pregnancy & Functions of Placenta-1Documento31 páginasPhysiology of Pregnancy & Functions of Placenta-1Ajit ShahAún no hay calificaciones
- Contraception S7 BDocumento14 páginasContraception S7 BArsh KaiwanAún no hay calificaciones
- Embryology Lecture Note 2Documento19 páginasEmbryology Lecture Note 2jestreametefiaAún no hay calificaciones
- Normal & Abnormal PuerperiumDocumento43 páginasNormal & Abnormal PuerperiumkazugawaAún no hay calificaciones
- Path o PhysioDocumento5 páginasPath o Physiomitzi019Aún no hay calificaciones
- Maternal and Child Health IDocumento772 páginasMaternal and Child Health Ikarendelarosa06100% (6)
- TUTORIALDocumento49 páginasTUTORIALAna Abadi Al IndAún no hay calificaciones
- Endocrinology of PregnancyDocumento68 páginasEndocrinology of PregnancySht SristiAún no hay calificaciones
- Infertility GuideDocumento24 páginasInfertility GuideDeepa ThomasAún no hay calificaciones
- Hydatidiform Mole-Is A Type of Gestational Trophoblastic Neoplasm ThatDocumento4 páginasHydatidiform Mole-Is A Type of Gestational Trophoblastic Neoplasm ThatjhelabooAún no hay calificaciones
- Pregnancy 1Documento70 páginasPregnancy 1Annapurna DangetiAún no hay calificaciones
- Anatomy and Physiology IIDocumento129 páginasAnatomy and Physiology IIkenmanikeseAún no hay calificaciones
- Objectives: at The End of This Session The Students Will Be Able ToDocumento33 páginasObjectives: at The End of This Session The Students Will Be Able ToPeachy HeartsAún no hay calificaciones
- MaternalDocumento41 páginasMaternalUc_tweenAún no hay calificaciones
- NCM 107 Lesson 5Documento6 páginasNCM 107 Lesson 5Geanne MananguAún no hay calificaciones
- Problem No.1Documento34 páginasProblem No.1ayesha bgAún no hay calificaciones
- Physiology of Female Reproductive SystemDocumento57 páginasPhysiology of Female Reproductive SystemIshaqAún no hay calificaciones
- Selecting Male Or Female Child Here's How It Works - Based On The Teachings Of Dr. Andrew Huberman: A Guide To Gender SelectionDe EverandSelecting Male Or Female Child Here's How It Works - Based On The Teachings Of Dr. Andrew Huberman: A Guide To Gender SelectionAún no hay calificaciones
- Menstrual Cycle Related Disorders: Volume 7: Frontiers in Gynecological EndocrinologyDe EverandMenstrual Cycle Related Disorders: Volume 7: Frontiers in Gynecological EndocrinologySarah L. BergaAún no hay calificaciones
- TrunkDocumento86 páginasTrunkdr_asalehAún no hay calificaciones
- How To Deal WithDocumento65 páginasHow To Deal Withdr_asalehAún no hay calificaciones
- Examination of TheDocumento29 páginasExamination of Thedr_asalehAún no hay calificaciones
- Knee.www.1aim.netDocumento34 páginasKnee.www.1aim.netdr_asalehAún no hay calificaciones
- LongDocumento64 páginasLongdr_asalehAún no hay calificaciones
- Elbow WristDocumento59 páginasElbow Wristdr_asalehAún no hay calificaciones
- OrthopedicDocumento71 páginasOrthopedicdr_asalehAún no hay calificaciones
- Hip.www.1aim.netDocumento60 páginasHip.www.1aim.netdr_asaleh100% (1)
- Injuries Around TheDocumento48 páginasInjuries Around Thedr_asalehAún no hay calificaciones
- Thoracic CavityDocumento30 páginasThoracic Cavitydr_asalehAún no hay calificaciones
- Upper ExtremityDocumento33 páginasUpper Extremitydr_asalehAún no hay calificaciones
- The Lower Limb: Pelvis, Thigh, Leg and FootDocumento27 páginasThe Lower Limb: Pelvis, Thigh, Leg and Footdr_asaleh100% (1)
- Bone JointDocumento57 páginasBone Jointdr_asalehAún no hay calificaciones
- Contents of PelvisDocumento38 páginasContents of Pelvisdr_asalehAún no hay calificaciones
- Head and NeckDocumento41 páginasHead and Neckdr_asalehAún no hay calificaciones
- Skull, Brain, CNDocumento60 páginasSkull, Brain, CNdr_asaleh100% (1)
- AbdomenDocumento11 páginasAbdomendr_asalehAún no hay calificaciones
- Head and NeckDocumento41 páginasHead and Neckdr_asalehAún no hay calificaciones
- Bones, Joints, MusclesDocumento37 páginasBones, Joints, Musclesdr_asalehAún no hay calificaciones
- Anatomy Lecture1Documento47 páginasAnatomy Lecture1dr_asalehAún no hay calificaciones
- Artries and VeinsDocumento25 páginasArtries and Veinsdr_asalehAún no hay calificaciones
- Infertility IVDocumento46 páginasInfertility IVdr_asalehAún no hay calificaciones
- Infertility IIIDocumento72 páginasInfertility IIIdr_asalehAún no hay calificaciones
- D. NegligenceDocumento11 páginasD. NegligenceKing GeorgeAún no hay calificaciones
- Femael Infertility PDFDocumento9 páginasFemael Infertility PDFAyadPalaniAún no hay calificaciones
- Estrogen Dominance Part 2 TherapeuticsDocumento34 páginasEstrogen Dominance Part 2 TherapeuticsAnthony De PontesAún no hay calificaciones
- The Ultimate Guide To FertilityDocumento32 páginasThe Ultimate Guide To FertilityMirjana14Aún no hay calificaciones
- Grade 10 Science Quarter 3Documento23 páginasGrade 10 Science Quarter 3Mary Cuevas (Ari)Aún no hay calificaciones
- Dental Education Program StudyDocumento5 páginasDental Education Program StudySaravanan SaravanankAún no hay calificaciones
- Pubertal Development: Question FDocumento19 páginasPubertal Development: Question FHARPREETAún no hay calificaciones
- RahimjindaniDocumento14 páginasRahimjindaniRahim JINDANIAún no hay calificaciones
- Mdcat Crash Test 1 BiologyDocumento8 páginasMdcat Crash Test 1 BiologyMUHAMMAD NOMAN SALEEMAún no hay calificaciones
- Third Periodical Test - Science 10 ANS KEYDocumento4 páginasThird Periodical Test - Science 10 ANS KEYMerlita CahuloganAún no hay calificaciones
- Midwifery Quiz Q&ADocumento71 páginasMidwifery Quiz Q&AKZAún no hay calificaciones
- Module 2 The Human Reproductive Anatomy and PhysiologyDocumento27 páginasModule 2 The Human Reproductive Anatomy and PhysiologyJhunna Talangan100% (1)
- Class XII Biology Sample Question Paper (Term I) 2021-22Documento20 páginasClass XII Biology Sample Question Paper (Term I) 2021-22Xyz XyzAún no hay calificaciones
- Abnormal Menstruations AUB and Dysmenorrhea: Abebe C (MD)Documento34 páginasAbnormal Menstruations AUB and Dysmenorrhea: Abebe C (MD)adam0% (1)
- 3º Eso Bquestionnaire Unit 7 - Adrián GarcíaDocumento4 páginas3º Eso Bquestionnaire Unit 7 - Adrián GarcíaBot 007Aún no hay calificaciones
- Estrus Induction in Dogs - Approaches, Protocols and Applications - WSAVA2005 - VINDocumento7 páginasEstrus Induction in Dogs - Approaches, Protocols and Applications - WSAVA2005 - VINMuhammad FaheemAún no hay calificaciones
- Male and Female Radiographic ProceduresDocumento5 páginasMale and Female Radiographic ProceduresKaye A. JardinicoAún no hay calificaciones
- Human ReproductionDocumento21 páginasHuman ReproductionShazia KhatoonAún no hay calificaciones