También podría gustarte
- Handbook of Current and Novel Protocols for the Treatment of InfertilityDe EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanAún no hay calificaciones
- Overview of Hemolytic Disease of Fetus and Newborn Erythroblastosis FetalisDocumento3 páginasOverview of Hemolytic Disease of Fetus and Newborn Erythroblastosis FetalisEditor IJTSRDAún no hay calificaciones
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesDe EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesAún no hay calificaciones
- DVT Blok 4.1Documento67 páginasDVT Blok 4.1Dz Putra100% (1)
- Blood TranfusionDocumento3 páginasBlood Tranfusionkeenoxky100% (1)
- 9fetal Well Being in PregnancyDocumento10 páginas9fetal Well Being in PregnancyuouoAún no hay calificaciones
- Aiims Neonatology 2012 PROTOCOL PDFDocumento245 páginasAiims Neonatology 2012 PROTOCOL PDFAnisur RahmanAún no hay calificaciones
- Periodic Health Examination national guideline وقايهDocumento56 páginasPeriodic Health Examination national guideline وقايهMohammed AbdulbaqiAún no hay calificaciones
- What Is Erythroblastosis Fetalis?: Red Blood CellsDocumento5 páginasWhat Is Erythroblastosis Fetalis?: Red Blood CellsMonalisa ParidaAún no hay calificaciones
- Neuroblastoma My Lecture 2011Documento153 páginasNeuroblastoma My Lecture 2011Wael ElsawyAún no hay calificaciones
- Comparison of Growth Pattern in Neonates On BreastDocumento7 páginasComparison of Growth Pattern in Neonates On BreastOman SantosoAún no hay calificaciones
- Trail of LaborDocumento5 páginasTrail of LaborNithiya NadesanAún no hay calificaciones
- WHO Labour Care GuideDocumento34 páginasWHO Labour Care GuideAnkita Singh100% (1)
- The Complete Blood Count Is The Calculation of The Cellular (Formed Elements) of BloodDocumento26 páginasThe Complete Blood Count Is The Calculation of The Cellular (Formed Elements) of BloodNabard MhammadAún no hay calificaciones
- LDRPDocumento20 páginasLDRPAnonymous ibmeej9Aún no hay calificaciones
- Wash OutDocumento11 páginasWash OutErick CorputtyAún no hay calificaciones
- Prevalence of Anemia Among Adolescent GirlsDocumento6 páginasPrevalence of Anemia Among Adolescent GirlsYolanda SimamoraAún no hay calificaciones
- Practice Essentials: DefinitionsDocumento5 páginasPractice Essentials: DefinitionsNovita sariAún no hay calificaciones
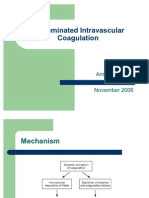
- Disseminated Intravascular CoagulationDocumento12 páginasDisseminated Intravascular CoagulationMunish Dogra100% (1)
- Exchange TransfusionDocumento9 páginasExchange TransfusiondewpraAún no hay calificaciones
- Cardiotocograph (CTG) Interpretation and ResponseDocumento23 páginasCardiotocograph (CTG) Interpretation and ResponseAndi Farid AAún no hay calificaciones
- Assisting Bone Marrow Aspiration DraftDocumento6 páginasAssisting Bone Marrow Aspiration Draftabcde pwnjabiAún no hay calificaciones
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocumento45 páginasMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيAún no hay calificaciones
- Antenatal & Postnatal Care: 1. General InformationDocumento7 páginasAntenatal & Postnatal Care: 1. General InformationanishnithaAún no hay calificaciones
- Neonatal Exchange Transfusion (Neonatal)Documento8 páginasNeonatal Exchange Transfusion (Neonatal)Muhammad ShahbazAún no hay calificaciones
- Hiv in PregnancyDocumento98 páginasHiv in PregnancyAkrit DahalAún no hay calificaciones
- Neonatal ProceduresDocumento74 páginasNeonatal ProceduresIbrahim Sabra100% (1)
- Etiology PPPDocumento24 páginasEtiology PPPCresty Estalilla100% (1)
- SP30 Neonatal Umbilical Vessel Catherization (Neonatal)Documento13 páginasSP30 Neonatal Umbilical Vessel Catherization (Neonatal)Ritzjerald Christer Abrena PahilanAún no hay calificaciones
- A Study To Assess The Knowledge of Mothers Regarding Weaning Among Children 6 Months To 2 Years of Age in Selected Rural Areas of Punjab IndiaDocumento3 páginasA Study To Assess The Knowledge of Mothers Regarding Weaning Among Children 6 Months To 2 Years of Age in Selected Rural Areas of Punjab IndiaIJARP PublicationsAún no hay calificaciones
- HydronephrosisDocumento2 páginasHydronephrosisGanis RyAún no hay calificaciones
- Retinopathy of Prematurity (ROP) - 2019Documento14 páginasRetinopathy of Prematurity (ROP) - 2019Suhail RafikAún no hay calificaciones
- WelcomeDocumento103 páginasWelcomeLyka BernalAún no hay calificaciones
- Gynecological Operation and Nursing ManagementDocumento29 páginasGynecological Operation and Nursing Managementhawra alsaadAún no hay calificaciones
- A Study To Assess Effectiveness of Information Booklet Regarding Use of Partograph Among Midwives Working in Labour Room of Selected Hospital of Bhopal M.PDocumento8 páginasA Study To Assess Effectiveness of Information Booklet Regarding Use of Partograph Among Midwives Working in Labour Room of Selected Hospital of Bhopal M.PEditor IJTSRDAún no hay calificaciones
- Kangeroo Care Final 1Documento22 páginasKangeroo Care Final 1api-438174007Aún no hay calificaciones
- Nosocomial Infections in NewbornsDocumento10 páginasNosocomial Infections in NewbornsAntony Rose AbyAún no hay calificaciones
- Amnio ReductionDocumento5 páginasAmnio ReductionNovhy Ganggut100% (1)
- Follow-upoftheNICUPatient Medscape FormatDocumento65 páginasFollow-upoftheNICUPatient Medscape FormatJohn ParudaAún no hay calificaciones
- Specimen Collection MicrobiologyDocumento25 páginasSpecimen Collection MicrobiologyHartiniAún no hay calificaciones
- Hiv in Pregnant WomenDocumento33 páginasHiv in Pregnant WomenWill CheahAún no hay calificaciones
- Renal CancerDocumento34 páginasRenal CancerArya100% (1)
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocumento31 páginasNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanAún no hay calificaciones
- Disease Condition:: Hyperemsis Gravidarum: DefinitionDocumento4 páginasDisease Condition:: Hyperemsis Gravidarum: DefinitionPriyanka JohnAún no hay calificaciones
- Hellp Syndrome: Prepared By: Jamie Niña Faye CDocumento10 páginasHellp Syndrome: Prepared By: Jamie Niña Faye CJamie DyAún no hay calificaciones
- RH IcompatibilityDocumento3 páginasRH IcompatibilitySourabh SharafAún no hay calificaciones
- MusQan National Quality Assurance Standards and Assessment Tools For DH and CHCDocumento274 páginasMusQan National Quality Assurance Standards and Assessment Tools For DH and CHCRahul JalauniaAún no hay calificaciones
- Assisting in Papanicolaou SmearDocumento13 páginasAssisting in Papanicolaou SmearRika Mae100% (1)
- Advance Seminar 2 2017Documento22 páginasAdvance Seminar 2 2017Shreyas Walvekar0% (1)
- CPG Management of Neonatal Jaundice (Second Edition)Documento62 páginasCPG Management of Neonatal Jaundice (Second Edition)umiraihana1100% (1)
- Icterus, HiperbilirubinemiaDocumento3 páginasIcterus, HiperbilirubinemiameidyAún no hay calificaciones
- Skill Laboratory Practice Module: Block: Reproductive System: 10 Topic: Pap SmearDocumento5 páginasSkill Laboratory Practice Module: Block: Reproductive System: 10 Topic: Pap SmearMuthiana Rizky0% (1)
- Rational Blood Transfusion in Infant and ChildrenDocumento37 páginasRational Blood Transfusion in Infant and ChildrenBayu KurniawanAún no hay calificaciones
- Management of Breast FeedingDocumento17 páginasManagement of Breast FeedingUday KumarAún no hay calificaciones
- Instrumental and Distructive DeliveryDocumento66 páginasInstrumental and Distructive DeliveryDagnachew kasayeAún no hay calificaciones
- Health Management Information SystemDocumento6 páginasHealth Management Information SystemSSERWADDA ENOCK100% (1)
- Lecture Notes On AphDocumento41 páginasLecture Notes On AphEyob MizanAún no hay calificaciones
- RH D Immunoglobulin (Anti-D)Documento4 páginasRH D Immunoglobulin (Anti-D)Ywagar YwagarAún no hay calificaciones
- Antibiotic Stewardship in Neonatal SepsisDocumento41 páginasAntibiotic Stewardship in Neonatal SepsisyusahanaAún no hay calificaciones
- Poly and OligohydramniosDocumento39 páginasPoly and OligohydramniosMohamed Atef MohamedAún no hay calificaciones
- EKG Rhythms2 PDFDocumento7 páginasEKG Rhythms2 PDFAya KamajayaAún no hay calificaciones
- CORNEADocumento59 páginasCORNEAAya KamajayaAún no hay calificaciones
- Urinary Tract PhysiologykulDocumento72 páginasUrinary Tract PhysiologykulAya KamajayaAún no hay calificaciones
- 10 Kuliah PLACENTADocumento33 páginas10 Kuliah PLACENTAAya KamajayaAún no hay calificaciones
- Cliniskill MasteryDocumento14 páginasCliniskill MasteryAya KamajayaAún no hay calificaciones
- HandBook of Pathology and PathoPhysiology of CardioVascularDocumento321 páginasHandBook of Pathology and PathoPhysiology of CardioVascularNurwahidah Moh WahiAún no hay calificaciones
- The Plant CellDocumento22 páginasThe Plant CellLuna Scorpius0% (1)
- The Theater of Anatomy - The Anatomical Preparations of Honore Fragonard PDFDocumento18 páginasThe Theater of Anatomy - The Anatomical Preparations of Honore Fragonard PDFFrancisco SantosAún no hay calificaciones
- History of Renal Neoplasia: Brett Delahunt MD Frcpa FrcpathDocumento5 páginasHistory of Renal Neoplasia: Brett Delahunt MD Frcpa FrcpathrizkaAún no hay calificaciones
- Shaukat Khanum Memorial Cancer Hospital & Research Centre: SPC Nature: SPC SiteDocumento3 páginasShaukat Khanum Memorial Cancer Hospital & Research Centre: SPC Nature: SPC SiteMisum AliAún no hay calificaciones
- Stele Types - The Arrangement of Xylem and Phloem in Stems, Rooots, and AxesDocumento30 páginasStele Types - The Arrangement of Xylem and Phloem in Stems, Rooots, and AxesYashica LalAún no hay calificaciones
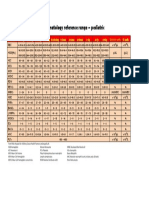
- Hematology Reference RangeDocumento1 páginaHematology Reference RangeNheeya WarzAún no hay calificaciones
- Anatomy and Physiology of Male Reproductive SystemDocumento8 páginasAnatomy and Physiology of Male Reproductive SystemAdor AbuanAún no hay calificaciones
- Histological Variants:: PathogenesisDocumento2 páginasHistological Variants:: PathogenesisPravin KumarAún no hay calificaciones
- Top 10 Acupuncture Points and ProtocolsDocumento13 páginasTop 10 Acupuncture Points and ProtocolsJaikanth MuthukumaraswamyAún no hay calificaciones
- A Detailed Lesson Plan in Science VIDocumento5 páginasA Detailed Lesson Plan in Science VIJose Anthony AlmoceraAún no hay calificaciones
- Neutralization, Hemolysis and Complement Fixation: Group 9 Megino, Elvin Maturgo, Kenneth Reyes, Patricia Vergara, CyrilDocumento42 páginasNeutralization, Hemolysis and Complement Fixation: Group 9 Megino, Elvin Maturgo, Kenneth Reyes, Patricia Vergara, CyrilPatty ReyesAún no hay calificaciones
- Introduction To Dental Anatomy (Dental Anatomy, Physiology and Occlusion) Part 2Documento1 páginaIntroduction To Dental Anatomy (Dental Anatomy, Physiology and Occlusion) Part 2Hicham KarrouchiAún no hay calificaciones
- Bladder AnatomuDocumento1 páginaBladder AnatomuCarlotta ranalliAún no hay calificaciones
- Antibody EngineeringDocumento14 páginasAntibody EngineeringJholina Aure ReyesAún no hay calificaciones
- notice-EVS Class 5 U1 T1 WSDocumento23 páginasnotice-EVS Class 5 U1 T1 WSGovind RajAún no hay calificaciones
- Pathophysiology AML DiagramDocumento4 páginasPathophysiology AML DiagramKlerra Hope60% (5)
- Biochem Experiment 3Documento3 páginasBiochem Experiment 3Julius Memeg PanayoAún no hay calificaciones
- Chapter 7 ReviewDocumento2 páginasChapter 7 ReviewRonaldAún no hay calificaciones
- Lesson Exemplar in ScienceDocumento7 páginasLesson Exemplar in ScienceMary Jane Angeles GarciaAún no hay calificaciones
- Gamete Formation in Animals PDFDocumento5 páginasGamete Formation in Animals PDFStarlight 101100% (1)
- FNA Soft TX TuDocumento74 páginasFNA Soft TX TufadoAún no hay calificaciones
- AVP Palatine Ulcers Article PDFDocumento5 páginasAVP Palatine Ulcers Article PDFartzain1991Aún no hay calificaciones
- Rosemary Estrada - Histology Lab NotebookDocumento12 páginasRosemary Estrada - Histology Lab NotebookRosemary EstradaAún no hay calificaciones
- Erythema MultiformeDocumento5 páginasErythema MultiformeNicco MarantsonAún no hay calificaciones
- Chapter 4Documento17 páginasChapter 4JohnAún no hay calificaciones
- Physiology and Its Central Principle: Homeostasis With Thad WilsonDocumento17 páginasPhysiology and Its Central Principle: Homeostasis With Thad WilsonVathana SorAún no hay calificaciones
- Hematology PPT 1Documento287 páginasHematology PPT 1TarishiMalikAún no hay calificaciones
- AP Psych 2.3 Notes - Nervous and Endocrine SystemDocumento2 páginasAP Psych 2.3 Notes - Nervous and Endocrine SystemIan BurtAún no hay calificaciones
- Ghid Plex Brahial Conturaj PDFDocumento7 páginasGhid Plex Brahial Conturaj PDFMiruna MafteiAún no hay calificaciones
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeDe EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeAún no hay calificaciones
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouDe EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouAún no hay calificaciones
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDe EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisCalificación: 3 de 5 estrellas3/5 (2)
- What to Expect When You’re Expecting (5th Edition)De EverandWhat to Expect When You’re Expecting (5th Edition)Calificación: 5 de 5 estrellas5/5 (1)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDe EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeCalificación: 3.5 de 5 estrellas3.5/5 (13)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayDe EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayCalificación: 4.5 de 5 estrellas4.5/5 (3)
- Reclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledgeDe EverandReclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledgeCalificación: 5 de 5 estrellas5/5 (16)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersDe EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersCalificación: 4.5 de 5 estrellas4.5/5 (72)
- Skinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!De EverandSkinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!Calificación: 3.5 de 5 estrellas3.5/5 (489)
- Natural Hospital Birth: The Best of Both WorldsDe EverandNatural Hospital Birth: The Best of Both WorldsCalificación: 5 de 5 estrellas5/5 (33)
- ADHD Women: A Holistic Approach To ADHD ManagementDe EverandADHD Women: A Holistic Approach To ADHD ManagementCalificación: 5 de 5 estrellas5/5 (4)
- Pregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!De EverandPregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!Calificación: 5 de 5 estrellas5/5 (1)
- Essential Labor: Mothering as Social ChangeDe EverandEssential Labor: Mothering as Social ChangeCalificación: 4 de 5 estrellas4/5 (25)
- Awakening Fertility: The Essential Art of Preparing for PregnancyDe EverandAwakening Fertility: The Essential Art of Preparing for PregnancyCalificación: 4.5 de 5 estrellas4.5/5 (36)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.De EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Calificación: 3.5 de 5 estrellas3.5/5 (7)
- Intoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingDe EverandIntoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingCalificación: 5 de 5 estrellas5/5 (1)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenDe EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenCalificación: 4 de 5 estrellas4/5 (154)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondDe EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondCalificación: 4.5 de 5 estrellas4.5/5 (39)
- Period Power: Harness Your Hormones and Get Your Cycle Working For YouDe EverandPeriod Power: Harness Your Hormones and Get Your Cycle Working For YouCalificación: 4 de 5 estrellas4/5 (25)
- First Time Dad: The Ultimate Guide for New Dads about Pregnancy Preparation and Childbirth - Advice, Facts, Tips, and Stories for First Time Fathers!De EverandFirst Time Dad: The Ultimate Guide for New Dads about Pregnancy Preparation and Childbirth - Advice, Facts, Tips, and Stories for First Time Fathers!Calificación: 5 de 5 estrellas5/5 (21)
- The Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysDe EverandThe Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysCalificación: 4.5 de 5 estrellas4.5/5 (5)
- The Cycle Syncing Handbook: Identify Hormonal Patterns, Build Holistic Habits, and Embrace the Power of Your Menstrual CycleDe EverandThe Cycle Syncing Handbook: Identify Hormonal Patterns, Build Holistic Habits, and Embrace the Power of Your Menstrual CycleAún no hay calificaciones
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodDe EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodCalificación: 5 de 5 estrellas5/5 (33)
- The Vegan-Keto Diet Meal Plan: Unexpected Uses for the Ketogenic Diet RecipesDe EverandThe Vegan-Keto Diet Meal Plan: Unexpected Uses for the Ketogenic Diet RecipesCalificación: 5 de 5 estrellas5/5 (1)
- WomanCode: Perfect Your Cycle, Amplify Your Fertility, Supercharge Your Sex Drive, and Become a Power SourceDe EverandWomanCode: Perfect Your Cycle, Amplify Your Fertility, Supercharge Your Sex Drive, and Become a Power SourceCalificación: 4.5 de 5 estrellas4.5/5 (91)
- The Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthDe EverandThe Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthCalificación: 4.5 de 5 estrellas4.5/5 (21)
- I'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeDe EverandI'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeCalificación: 4 de 5 estrellas4/5 (15)
- I'm So Effing Hungry: Why We Crave What We Crave – and What to Do About ItDe EverandI'm So Effing Hungry: Why We Crave What We Crave – and What to Do About ItAún no hay calificaciones