También podría gustarte
- Case Presentation On Autosomal Recessive Polycystic Kidney Disease (ARPKD)Documento15 páginasCase Presentation On Autosomal Recessive Polycystic Kidney Disease (ARPKD)narseya100% (1)
- Mechanisms Case StudyDocumento13 páginasMechanisms Case Studyshane_tin143Aún no hay calificaciones
- Case Studybleeding Biliary AtresiaDocumento13 páginasCase Studybleeding Biliary Atresialawrence tayamAún no hay calificaciones
- Case Study On Meninomyocele (Repaired) PDocumento29 páginasCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- CPD, Dystocia, Fetal Distress OutputDocumento8 páginasCPD, Dystocia, Fetal Distress OutputJohn Dave AbranAún no hay calificaciones
- Febrile Seizures NCPDocumento9 páginasFebrile Seizures NCPNurul IrhamnaAún no hay calificaciones
- Case Report Tetralogy of Fallot-CompleteDocumento72 páginasCase Report Tetralogy of Fallot-CompleteMaydis stigmaAún no hay calificaciones
- Case Studies - Tetralogy of FallotDocumento16 páginasCase Studies - Tetralogy of FallotKunwar Sidharth SaurabhAún no hay calificaciones
- Aklan State University Nursing Readings on Pyloric StenosisDocumento5 páginasAklan State University Nursing Readings on Pyloric Stenosisensoooooooooo100% (1)
- Jaundice NeonatalDocumento26 páginasJaundice Neonatalhunk2662Aún no hay calificaciones
- Beta ThalaDocumento2 páginasBeta ThalaAngie LamoAún no hay calificaciones
- Duphaston PDFDocumento4 páginasDuphaston PDFmarcusjanaAún no hay calificaciones
- TH THDocumento29 páginasTH THK RAVI KUMARAún no hay calificaciones
- The Components of Labor and DeliveryDocumento4 páginasThe Components of Labor and DeliveryGwyneth Nicole BudayAún no hay calificaciones
- Meconium Aspiration Syndrome: DR Bob KlajoDocumento17 páginasMeconium Aspiration Syndrome: DR Bob KlajoBob John100% (1)
- A Case Study On Cns InfectionDocumento33 páginasA Case Study On Cns InfectionMarie Joy Luczon100% (2)
- Abruptio Placentae Case StudyDocumento36 páginasAbruptio Placentae Case StudyisaacdarylAún no hay calificaciones
- Placenta Previa: Causes, Symptoms and TreatmentDocumento9 páginasPlacenta Previa: Causes, Symptoms and TreatmentSanket TelangAún no hay calificaciones
- Rh Factor and Pregnancy: Understanding Rh IncompatibilityDocumento22 páginasRh Factor and Pregnancy: Understanding Rh IncompatibilityDrPreeti Thakur ChouhanAún no hay calificaciones
- MECONIUM Aspiration SyndromeDocumento37 páginasMECONIUM Aspiration SyndromekamalaAún no hay calificaciones
- Ophthalmia NeonatorumDocumento19 páginasOphthalmia NeonatorumSanthu Tvm100% (1)
- Gastroschisis Final PresentationDocumento43 páginasGastroschisis Final PresentationlhedavenAún no hay calificaciones
- Nicu ReportDocumento18 páginasNicu ReportKabita KarakAún no hay calificaciones
- Post MaturityDocumento5 páginasPost MaturityBa BamAún no hay calificaciones
- Fetal Distress Case DiscussionDocumento55 páginasFetal Distress Case DiscussionHafsah G.Aún no hay calificaciones
- Observational Case Study of A NewbornDocumento2 páginasObservational Case Study of A NewbornCheska Mae PalicAún no hay calificaciones
- Nursing Consideration For A Hospitalized ChildDocumento24 páginasNursing Consideration For A Hospitalized Childsally limAún no hay calificaciones
- CP On Abrutio PlacentaDocumento13 páginasCP On Abrutio PlacentaUsha DeviAún no hay calificaciones
- Intrauterine Growth Restriction IUGRDocumento8 páginasIntrauterine Growth Restriction IUGRJyoti Prem UttamAún no hay calificaciones
- Tracheo-Oesophageal FistulaDocumento19 páginasTracheo-Oesophageal Fistularajan kumar100% (3)
- Neonatal SepsisDocumento44 páginasNeonatal SepsisIsabel Barredo Del MundoAún no hay calificaciones
- Session13 - Endometrial CaDocumento27 páginasSession13 - Endometrial CaCHALIE MEQUAún no hay calificaciones
- Pediatric Imperforate Anus - Background, Pathophysiology, EpidemiologyDocumento4 páginasPediatric Imperforate Anus - Background, Pathophysiology, EpidemiologyYehuda Agus SantosoAún no hay calificaciones
- Ectopic Pregnancy CasiaDocumento16 páginasEctopic Pregnancy CasiaMarie Ashley CasiaAún no hay calificaciones
- EsophagogastroduodenosDocumento6 páginasEsophagogastroduodenosdrnareshkumar3281Aún no hay calificaciones
- The Neonate at 24 To 48 Hours Following Early DischargeDocumento8 páginasThe Neonate at 24 To 48 Hours Following Early Dischargenursereview100% (2)
- Final Case Study-Bili (ReVISED)Documento35 páginasFinal Case Study-Bili (ReVISED)malentot100% (1)
- Grand ReportsDocumento60 páginasGrand ReportsfilchibuffAún no hay calificaciones
- Biliary AtresiaDocumento25 páginasBiliary Atresiajulius billiAún no hay calificaciones
- KamanJan ChloroquineDocumento3 páginasKamanJan Chloroquinekimberly_caberteAún no hay calificaciones
- Nursing Care Plan for Subarachnoid HemorrhageDocumento46 páginasNursing Care Plan for Subarachnoid HemorrhageShitaljit IromAún no hay calificaciones
- Case Presentation HydrocephalusDocumento48 páginasCase Presentation HydrocephalusSu Osman50% (2)
- Bronchial Asthma in ChildrenDocumento19 páginasBronchial Asthma in ChildrenIvanAún no hay calificaciones
- Type B (Hib) Vaccine: Haemophilus InfluenzaeDocumento2 páginasType B (Hib) Vaccine: Haemophilus InfluenzaeEnce MalatambanAún no hay calificaciones
- Acute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) NovemberDocumento28 páginasAcute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) Novemberزكريا عمرAún no hay calificaciones
- Febrile ConvulsionDocumento20 páginasFebrile ConvulsionnoblefxAún no hay calificaciones
- PretermDocumento11 páginasPretermAlma Gobaleza100% (2)
- Failure To ThriveDocumento93 páginasFailure To ThriveMuhammad Siddiq100% (1)
- GastroschisisDocumento19 páginasGastroschisiskunaidongAún no hay calificaciones
- Tuberculosis and Nephrotic Syndrome in a ChildDocumento34 páginasTuberculosis and Nephrotic Syndrome in a ChildAldo YustiantoAún no hay calificaciones
- Case Study 1: Nicole: 1. Discuss The Significance of Nicole's Laboratory FindingsDocumento12 páginasCase Study 1: Nicole: 1. Discuss The Significance of Nicole's Laboratory FindingsClint NavarroAún no hay calificaciones
- Pre EclampsiaDocumento13 páginasPre EclampsiaEniamrahs DnalonAún no hay calificaciones
- Respiratory Distress Syndrome in A Premature BabyDocumento29 páginasRespiratory Distress Syndrome in A Premature BabyVissalini JayabalanAún no hay calificaciones
- Intussuseption and Hirschprung's DiseaseDocumento5 páginasIntussuseption and Hirschprung's DiseaseAris Magallanes100% (2)
- Febrile Seizure Case FileDocumento4 páginasFebrile Seizure Case Filehttps://medical-phd.blogspot.comAún no hay calificaciones
- Diabetes in PregnancyDocumento88 páginasDiabetes in PregnancyKathleenZunigaAún no hay calificaciones
- Neonatal JaundiceDocumento24 páginasNeonatal JaundiceJOSLINAún no hay calificaciones
- Multifetal Pregnancy: Amr Nadim, MDDocumento36 páginasMultifetal Pregnancy: Amr Nadim, MDsharenAún no hay calificaciones
- PEDIATRICS CASEDocumento12 páginasPEDIATRICS CASEAmaetenAún no hay calificaciones
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAún no hay calificaciones
- FASCIOLADocumento1 páginaFASCIOLASharmaine SimonAún no hay calificaciones
- Owl AnalyzerDocumento1 páginaOwl AnalyzerSharmaine SimonAún no hay calificaciones
- Code SystemDocumento1 páginaCode SystemSharmaine SimonAún no hay calificaciones
- Obscure, and Interesting Information and Facts About MothersDocumento4 páginasObscure, and Interesting Information and Facts About MothersSharmaine SimonAún no hay calificaciones
- Wilms Tumor Signs & Symptoms by SystemDocumento3 páginasWilms Tumor Signs & Symptoms by SystemSharmaine SimonAún no hay calificaciones
- Surgical InstrumentsDocumento8 páginasSurgical InstrumentsSharmaine Simon91% (11)
- Diocletian Palace Split OrnamentsDocumento3 páginasDiocletian Palace Split OrnamentsPandexaAún no hay calificaciones
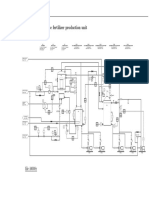
- Diagrama P ID Ammonium Nitrate Fertilizer Production Unit PDFDocumento1 páginaDiagrama P ID Ammonium Nitrate Fertilizer Production Unit PDFYecid Fabian AlvaradoAún no hay calificaciones
- DID 180 Standard Roller Chain: Roller Chains For Power TransmissionDocumento1 páginaDID 180 Standard Roller Chain: Roller Chains For Power TransmissionJhampol Rosales MuñozAún no hay calificaciones
- M.A Chaudary Greenhall OL Physics NotesDocumento139 páginasM.A Chaudary Greenhall OL Physics NotesArshad KhanAún no hay calificaciones
- The Following Describes The Competition Between Google and Amazon ForDocumento1 páginaThe Following Describes The Competition Between Google and Amazon Fortrilocksp SinghAún no hay calificaciones
- Enthalpy For Pyrolysis For Several Types of BiomassDocumento7 páginasEnthalpy For Pyrolysis For Several Types of BiomassSwiftTGSolutionsAún no hay calificaciones
- The Universal Treatise of Global Economic Common SenseDocumento727 páginasThe Universal Treatise of Global Economic Common SenseWilliam E. FieldsAún no hay calificaciones
- Georg Heym The Thief and Other Stories 1Documento110 páginasGeorg Heym The Thief and Other Stories 1Anna ShkodenkoAún no hay calificaciones
- ACCAF5 - Qbank2017 - by First Intuition Downloaded FromDocumento384 páginasACCAF5 - Qbank2017 - by First Intuition Downloaded FromAbdul Jabbar Al-Shaer100% (4)
- AQA Biology A-Level - Cell Cycle and Mitosis QPDocumento22 páginasAQA Biology A-Level - Cell Cycle and Mitosis QPMuffin CAún no hay calificaciones
- Salt in Crude AnalyserDocumento2 páginasSalt in Crude AnalyserJoko Setio PurnomoAún no hay calificaciones
- Activity 3. Measure of Central Tendency and QuantileDocumento2 páginasActivity 3. Measure of Central Tendency and QuantileRowena G. TenecioAún no hay calificaciones
- Net Change JDEWorld A73 16Documento82 páginasNet Change JDEWorld A73 16Manoj LugunAún no hay calificaciones
- Filters for Hydraulic ExcavatorsDocumento18 páginasFilters for Hydraulic ExcavatorsTan JaiAún no hay calificaciones
- Rule of Ultra Vires With Respect To The Power of A CompanyDocumento19 páginasRule of Ultra Vires With Respect To The Power of A CompanyAbbas HaiderAún no hay calificaciones
- A320 Flow PatternDocumento18 páginasA320 Flow PatternFritz Carlo MagpantayAún no hay calificaciones
- DSL Oral QuestionDocumento5 páginasDSL Oral QuestionAmit SangaleAún no hay calificaciones
- Experiment No 1 Preparation of CheeseDocumento5 páginasExperiment No 1 Preparation of CheeseArmiee InfiniteAún no hay calificaciones
- Como Agua para Chocolate English PDFDocumento2 páginasComo Agua para Chocolate English PDFDavidAún no hay calificaciones
- 2 Bedroom OfferDocumento17 páginas2 Bedroom OfferLaksh RameshAún no hay calificaciones
- Business Plan (Administrative Plan)Documento8 páginasBusiness Plan (Administrative Plan)Noorul Farah Ain0% (1)
- Biology 11th Edition Raven Test BankDocumento24 páginasBiology 11th Edition Raven Test BankAngelaLewisyqza100% (22)
- Table - 4 ST - Scheduled Tribe Female Headed Households Classified by Source and Location of Drinking Water and Availablity of Electricity and Latrine Table For IndiaDocumento100 páginasTable - 4 ST - Scheduled Tribe Female Headed Households Classified by Source and Location of Drinking Water and Availablity of Electricity and Latrine Table For IndiaAman GuptaAún no hay calificaciones
- Endocrine SeminarDocumento58 páginasEndocrine SeminarShahirah ShuhaimiAún no hay calificaciones
- EDUCADO Course Syllabus TTL BEEdDocumento14 páginasEDUCADO Course Syllabus TTL BEEdJoseph Gabriel Educado100% (1)
- Paper - Investing in Indonesian Pharmaceutical Companies in The Middle of Pandemic UncertaintyDocumento9 páginasPaper - Investing in Indonesian Pharmaceutical Companies in The Middle of Pandemic UncertaintyZuchrizal WinataAún no hay calificaciones
- BSR 512: Topic 2: Norehan Haji Mohd Noor Senior Lecturer Program of Building Surveying, Uitm PerakDocumento35 páginasBSR 512: Topic 2: Norehan Haji Mohd Noor Senior Lecturer Program of Building Surveying, Uitm PerakaremyulAún no hay calificaciones
- Volume/ Voice Modulation: Stage PresenceDocumento1 páginaVolume/ Voice Modulation: Stage PresenceQuerobin GampayonAún no hay calificaciones
- MODULE 1: Parts and Functions of Computers Basic Parts of ComputerDocumento31 páginasMODULE 1: Parts and Functions of Computers Basic Parts of ComputerSophia Shannon D. DeiparineAún no hay calificaciones
- ATB Riva Calzoni Gianluca RaseniDocumento35 páginasATB Riva Calzoni Gianluca RaseniDiana QuinteroAún no hay calificaciones