También podría gustarte
- CKC Epi EquationDocumento5 páginasCKC Epi EquationWael_Soliman_1373Aún no hay calificaciones
- Estimating Glomerular Filtration RateDocumento7 páginasEstimating Glomerular Filtration RateShirin SyailandiraAún no hay calificaciones
- Chronickidneydiseaseinthe Elderly: Thin Thin Maw,, Linda FriedDocumento14 páginasChronickidneydiseaseinthe Elderly: Thin Thin Maw,, Linda Friedkhangha.ptAún no hay calificaciones
- Interpretation of The eGFR Jul 07Documento8 páginasInterpretation of The eGFR Jul 07Danielcc LeeAún no hay calificaciones
- Cystatin: What Is Its RoleDocumento8 páginasCystatin: What Is Its RoleDwinita ViviantiAún no hay calificaciones
- Diagnosis and Management of Early Stage Diabetic Kidney DiseaseDocumento11 páginasDiagnosis and Management of Early Stage Diabetic Kidney DiseaseCentral Asian StudiesAún no hay calificaciones
- UACR GFR QuickReference 508Documento2 páginasUACR GFR QuickReference 508sarfraz_eeeAún no hay calificaciones
- Should We Continue To Use The Cockcroft-Gault Formula?: MinireviewDocumento15 páginasShould We Continue To Use The Cockcroft-Gault Formula?: MinireviewJesse Helmut Hansen-BartelAún no hay calificaciones
- Principle and Practice of CT in Cardiac AssessmentDocumento47 páginasPrinciple and Practice of CT in Cardiac AssessmentSofia KusumadewiAún no hay calificaciones
- Chronic Kidney Disease: Paul Cockwell Queen Elizabeth Hospital BirminghamDocumento44 páginasChronic Kidney Disease: Paul Cockwell Queen Elizabeth Hospital BirminghamDhruva PatelAún no hay calificaciones
- ASN 2019030238 FullDocumento21 páginasASN 2019030238 FullAnita SulistioAún no hay calificaciones
- AURORA: Is There A Role For Statin Therapy in Dialysis Patients?Documento4 páginasAURORA: Is There A Role For Statin Therapy in Dialysis Patients?Ravan WidiAún no hay calificaciones
- Gfi 163Documento5 páginasGfi 163trinda ireneAún no hay calificaciones
- Cystatin: What Is Its RoleDocumento8 páginasCystatin: What Is Its RolecmeytasAún no hay calificaciones
- Rosuvastatin Reduces Coronary Plaque in ASTEROID TrialDocumento12 páginasRosuvastatin Reduces Coronary Plaque in ASTEROID TrialSharmil IyapillaiAún no hay calificaciones
- Anticoagulação em Pctes Com FA e Demência AvançadaDocumento3 páginasAnticoagulação em Pctes Com FA e Demência AvançadaresidentespaliAún no hay calificaciones
- Evaluation of Prediabetes in High Risk Population of Kashmir ValleyDocumento5 páginasEvaluation of Prediabetes in High Risk Population of Kashmir ValleyIJAR JOURNALAún no hay calificaciones
- CKD - Drug DosingDocumento7 páginasCKD - Drug DosingRafaelAún no hay calificaciones
- Screening For CKD With eGFR Doubts and DangersDocumento6 páginasScreening For CKD With eGFR Doubts and Dangersanderson roberto oliveira de sousaAún no hay calificaciones
- DELIVER Primary Manuscript. N Engl J Med. 2022 - With VEEVADocumento10 páginasDELIVER Primary Manuscript. N Engl J Med. 2022 - With VEEVAzdmoorAún no hay calificaciones
- CKD COMPLICATIONSDocumento7 páginasCKD COMPLICATIONSmetaAún no hay calificaciones
- Cardiorenal Syndrome - Prognosis and Treatment - UpToDateDocumento23 páginasCardiorenal Syndrome - Prognosis and Treatment - UpToDateJoão Lucas MoraisAún no hay calificaciones
- Cardiorenal Outcomes in The CANVAS, DECLARE-TIMI 58, and EMPA-REG OUTCOME Trials - A Systematic ReviewDocumento9 páginasCardiorenal Outcomes in The CANVAS, DECLARE-TIMI 58, and EMPA-REG OUTCOME Trials - A Systematic ReviewVaibhav DafaleAún no hay calificaciones
- Chronic Kidney Disease: Rizki Aliana AgustinaDocumento85 páginasChronic Kidney Disease: Rizki Aliana AgustinaRofi IrmanAún no hay calificaciones
- Life Expectancy With Chronic Kidney Disease: An Educational ReviewDocumento6 páginasLife Expectancy With Chronic Kidney Disease: An Educational Reviewahmad faisolAún no hay calificaciones
- Chronic Kidney Disease (CKD) :: An Update For The Primary PhysicianDocumento57 páginasChronic Kidney Disease (CKD) :: An Update For The Primary PhysicianHigh EducationAún no hay calificaciones
- PDF 9Documento8 páginasPDF 9OulnstAún no hay calificaciones
- LDL cholesterol reduction effects by risk levelDocumento18 páginasLDL cholesterol reduction effects by risk levelhenryweiAún no hay calificaciones
- NAFLD and microalbuminuria in prediabetesDocumento4 páginasNAFLD and microalbuminuria in prediabetesBinaNuraeniAún no hay calificaciones
- CKD - Case StudyDocumento48 páginasCKD - Case StudyEdmond DontessAún no hay calificaciones
- Cystatin C As An Early Marker of Diabetic Nephropathy in Nigerian Adults With Type 2 DiabetesDocumento9 páginasCystatin C As An Early Marker of Diabetic Nephropathy in Nigerian Adults With Type 2 Diabetesijmb333Aún no hay calificaciones
- Nejmoa 2206286Documento10 páginasNejmoa 2206286Usmle StepAún no hay calificaciones
- The Total Cholesterol To High-Density Lipoprotein Cholesterol As A Predictor of Poor Outcomes in A Chinese Population With Acute Ischaemic StrokeDocumento6 páginasThe Total Cholesterol To High-Density Lipoprotein Cholesterol As A Predictor of Poor Outcomes in A Chinese Population With Acute Ischaemic StrokeRay HannaAún no hay calificaciones
- MPV as a Predictor of Retinopathy in DiabetesDocumento12 páginasMPV as a Predictor of Retinopathy in DiabetesHamid IqbalAún no hay calificaciones
- DELIVER Nejmoa2206286Documento10 páginasDELIVER Nejmoa2206286Anonymous oQtve4oAún no hay calificaciones
- Plaquetas en Hta No Dipper - 2010Documento5 páginasPlaquetas en Hta No Dipper - 2010Andres VelascoAún no hay calificaciones
- Papers: Normal Serum Aminotransferase Concentration and Risk of Mortality From Liver Diseases: Prospective Cohort StudyDocumento6 páginasPapers: Normal Serum Aminotransferase Concentration and Risk of Mortality From Liver Diseases: Prospective Cohort StudyahmedlakhaAún no hay calificaciones
- Impact of Empagliflozin On Right Ventricular Parameters and Function Among Patients With Type 2 DiabetesCardiovascular DiabetologyDocumento11 páginasImpact of Empagliflozin On Right Ventricular Parameters and Function Among Patients With Type 2 DiabetesCardiovascular Diabetologygabriela naranjoAún no hay calificaciones
- BMJ-PIT Patologi Klinik-Edward KSL-1Documento5 páginasBMJ-PIT Patologi Klinik-Edward KSL-1Novi RatnaAún no hay calificaciones
- Stop-Acei Trial Journal ClubDocumento3 páginasStop-Acei Trial Journal Clubapi-648891519Aún no hay calificaciones
- Freedom TrialDocumento34 páginasFreedom TrialDaniela DíazAún no hay calificaciones
- Chronic Kidney Disease (CKD) : Provider's Guide To Diagnose and Code CKDDocumento2 páginasChronic Kidney Disease (CKD) : Provider's Guide To Diagnose and Code CKDAry Rio PambudiAún no hay calificaciones
- Hipoalbumin 1 PDFDocumento4 páginasHipoalbumin 1 PDFWira ZulfikarAún no hay calificaciones
- Cholong It As 2016Documento2 páginasCholong It As 2016arieftamaAún no hay calificaciones
- Relation Between Kidney Function, Proteinuria, and Adverse OutcomesDocumento7 páginasRelation Between Kidney Function, Proteinuria, and Adverse OutcomesSelvakumar ChelliahAún no hay calificaciones
- Age +estimated+glomerular+filtration+rate+and+ejection+fraction+score+predicts+contrast-Induced+acute+kidney+injury+in+patients+with+diabetes+and+chronic+kidney+disease +insight+from+the+TRACK-D+studyDocumento5 páginasAge +estimated+glomerular+filtration+rate+and+ejection+fraction+score+predicts+contrast-Induced+acute+kidney+injury+in+patients+with+diabetes+and+chronic+kidney+disease +insight+from+the+TRACK-D+studyangga_darmawan26Aún no hay calificaciones
- Cancer OvariumDocumento16 páginasCancer OvariumDwi RahmawatiAún no hay calificaciones
- Leaflet SCOREDocumento2 páginasLeaflet SCOREAdeline DevitaAún no hay calificaciones
- Estimation of Glomerular Filtration Rate in South Asian Healthy Adult Kidney DonorsDocumento7 páginasEstimation of Glomerular Filtration Rate in South Asian Healthy Adult Kidney DonorsJoel KennedyAún no hay calificaciones
- 2016 Article 69Documento10 páginas2016 Article 69Rhowy Al-mu'izzahAún no hay calificaciones
- SGLT2 inhibitors may reduce cardiovascular risk in chronic kidney diseaseDocumento5 páginasSGLT2 inhibitors may reduce cardiovascular risk in chronic kidney diseasePablo SánchezAún no hay calificaciones
- 302 Cardiovascular Risk: AssessmentDocumento1 página302 Cardiovascular Risk: AssessmentLêHữuHoàiAún no hay calificaciones
- PCP in A Box - Module 1Documento43 páginasPCP in A Box - Module 1Fate ChanAún no hay calificaciones
- Prevalence of Anemia in Patients With Type 2 Diabetes Mellitus at Gandhinagar, Gujarat, IndiaDocumento5 páginasPrevalence of Anemia in Patients With Type 2 Diabetes Mellitus at Gandhinagar, Gujarat, Indiaayham luAún no hay calificaciones
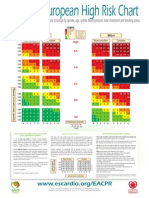
- 10 Year Risk of Fatal CVD in High Risk Regions of Europe by Gender, Age, Systolic Blood Pressure, Total Cholesterol and Smoking StatusDocumento2 páginas10 Year Risk of Fatal CVD in High Risk Regions of Europe by Gender, Age, Systolic Blood Pressure, Total Cholesterol and Smoking StatusCotovici Catana AlinaAún no hay calificaciones
- Chronic Kidney Disease: The BasicsDocumento56 páginasChronic Kidney Disease: The BasicsAlmas Safina KauserAún no hay calificaciones
- Intensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialDocumento4 páginasIntensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialSheebaAún no hay calificaciones
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2De EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2Aún no hay calificaciones
- Managing Cardiovascular Complications in DiabetesDe EverandManaging Cardiovascular Complications in DiabetesAún no hay calificaciones
- Case-Based Device Therapy for Heart FailureDe EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenAún no hay calificaciones
- Schizophrenia: Causes, Types, and Nursing CareDocumento32 páginasSchizophrenia: Causes, Types, and Nursing CareNasriah Macadato100% (1)
- Osmotic DiureticsDocumento30 páginasOsmotic Diureticsrhimineecat71100% (1)
- 6th Course For Somatosensory Rehabilitation of PainDocumento10 páginas6th Course For Somatosensory Rehabilitation of PainGerry OconnorAún no hay calificaciones
- Care of New BornDocumento25 páginasCare of New BornNirupama KsAún no hay calificaciones
- CrohnsDocumento19 páginasCrohnsLauren LevyAún no hay calificaciones
- Tartrazine Yellow: SynonymsDocumento11 páginasTartrazine Yellow: Synonymsbestread67Aún no hay calificaciones
- DSM OcdDocumento2 páginasDSM Ocdnmyza89Aún no hay calificaciones
- 09 SterilizationDocumento34 páginas09 Sterilizationitung2350% (2)
- Person-Centered Therapy - Wikipedia, The Free EncyclopediaDocumento4 páginasPerson-Centered Therapy - Wikipedia, The Free EncyclopediaMartin Levy100% (1)
- Anna Faust Resume 2021Documento2 páginasAnna Faust Resume 2021api-581442452Aún no hay calificaciones
- Absen Metod!!!Documento4 páginasAbsen Metod!!!Haris Pratama RebornAún no hay calificaciones
- Guideline PERKENI 2015Documento34 páginasGuideline PERKENI 2015Iin Citra Liana HasibuanAún no hay calificaciones
- Peptic UlcerDocumento4 páginasPeptic UlcerEris Abdul AzizAún no hay calificaciones
- Udaasi Aur Depression Ka Ilaj Kaise Kare Treatment in HindiDocumento6 páginasUdaasi Aur Depression Ka Ilaj Kaise Kare Treatment in HindiGovindAún no hay calificaciones
- Senior Project ProposalDocumento10 páginasSenior Project Proposalapi-384821983Aún no hay calificaciones
- Edgar Cayce On HealingDocumento132 páginasEdgar Cayce On Healinganca_dinca0% (1)
- Acute PancreatitisDocumento46 páginasAcute PancreatitisLew NianAún no hay calificaciones
- Blocked Goat Urolithiasis HandoutDocumento22 páginasBlocked Goat Urolithiasis Handoutapi-262327869100% (1)
- Plumbing Questionnaire 2Documento51 páginasPlumbing Questionnaire 2mcpayod100% (1)
- Micro Tech Endoscopy Product CatalogDocumento42 páginasMicro Tech Endoscopy Product CatalogyasuluAún no hay calificaciones
- DrugsDocumento17 páginasDrugsQais ShaikhAún no hay calificaciones
- Management of Patients With Gastric and Duodenal DisordersDocumento47 páginasManagement of Patients With Gastric and Duodenal DisordersJor GarciaAún no hay calificaciones
- Nasal Polyp Nasa Arsha Management Through Ayurveda A Single Case StudyDocumento4 páginasNasal Polyp Nasa Arsha Management Through Ayurveda A Single Case StudyEditor IJTSRDAún no hay calificaciones
- 09 Dialysis DataDocumento11 páginas09 Dialysis DataThinkingPinoyAún no hay calificaciones
- SEMINARDocumento19 páginasSEMINARTaiwoAún no hay calificaciones
- Nursing Practice QuestionsDocumento22 páginasNursing Practice QuestionsJune DumdumayaAún no hay calificaciones
- Unit 1: Consumer HealthDocumento23 páginasUnit 1: Consumer HealthGriffin AndersonAún no hay calificaciones
- Asthma: Setya Puspa Dewi AprilyaniDocumento19 páginasAsthma: Setya Puspa Dewi Aprilyaninadia kurnia100% (1)
- ImplantDocumento4 páginasImplantMohamed KudaihAún no hay calificaciones
- Hemolytic DiseaseDocumento10 páginasHemolytic DiseaseChino Paolo SamsonAún no hay calificaciones