También podría gustarte
- 04 Head Neck Lymph NodeDocumento17 páginas04 Head Neck Lymph Nodeamelia89212Aún no hay calificaciones
- Types of ComputerDocumento20 páginasTypes of ComputerMansoor Khan25% (4)
- Technique SummaryDocumento3 páginasTechnique SummaryMohammed Idriss AmirAún no hay calificaciones
- Procedures I Chapter 1 BontragerDocumento40 páginasProcedures I Chapter 1 BontragerMohammed Idriss AmirAún no hay calificaciones
- 2 DigitalDocumento25 páginas2 DigitalMohammed Idriss AmirAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Test Bank For Laboratory Manual For Seeleys Anatomy Physiology 11th Edition Eric Wise 3 DownloadDocumento69 páginasTest Bank For Laboratory Manual For Seeleys Anatomy Physiology 11th Edition Eric Wise 3 Downloadcaseyyoungtoekwmcfdi100% (25)
- Avian Skeletal System - EXtensionDocumento3 páginasAvian Skeletal System - EXtensionNagyeongAún no hay calificaciones
- Clavicle (Bone and Attachments) Flow ChartDocumento2 páginasClavicle (Bone and Attachments) Flow Chartshree niwasAún no hay calificaciones
- True NorthDocumento2 páginasTrue NorthtpAún no hay calificaciones
- Bone Structure and Function in 40 CharactersDocumento21 páginasBone Structure and Function in 40 CharactersMd Ahsanuzzaman PinkuAún no hay calificaciones
- Week 5 Skeletal SystemDocumento10 páginasWeek 5 Skeletal SystemKimberly Faye JuevesAún no hay calificaciones
- Exception Include Burst # of Spine, Some Lateral Wedge # and Extension Injuries of Cervical SpineDocumento29 páginasException Include Burst # of Spine, Some Lateral Wedge # and Extension Injuries of Cervical Spinebhavesh jain100% (2)
- Types and Features of Synovial JointsDocumento8 páginasTypes and Features of Synovial JointsSheena Mae AtienzaAún no hay calificaciones
- Processing of Temporomandibular Joint Dislocation Cases at Igd Rsud UNDATA PALU IN 2017-2018Documento4 páginasProcessing of Temporomandibular Joint Dislocation Cases at Igd Rsud UNDATA PALU IN 2017-2018Jamalul HikmahAún no hay calificaciones
- Endoskeleton of Frog (With Diagram) : The Endoskeleton Is Described Under Two Broad HeadsDocumento13 páginasEndoskeleton of Frog (With Diagram) : The Endoskeleton Is Described Under Two Broad HeadsMarielle AcojidoAún no hay calificaciones
- Bone, Joint and Soft TissueDocumento10 páginasBone, Joint and Soft Tissuesarguss14100% (2)
- Paranasal SinusDocumento51 páginasParanasal Sinusjosephwilliams_joeyAún no hay calificaciones
- Vanguard Instrument OptionsDocumento57 páginasVanguard Instrument OptionsBobAún no hay calificaciones
- Muscular System: Cardiac Muscle Skeletal MuscleDocumento10 páginasMuscular System: Cardiac Muscle Skeletal MuscleCherry Mae TapacionAún no hay calificaciones
- Arthritis, Spine Imaging, and Beyond - : Dr. Harun Gupta's TalkDocumento20 páginasArthritis, Spine Imaging, and Beyond - : Dr. Harun Gupta's TalkDonna MaharaniAún no hay calificaciones
- College of Veterinary Science Animal HusbandryDocumento174 páginasCollege of Veterinary Science Animal HusbandryabdulAún no hay calificaciones
- Bdol34 2Documento2 páginasBdol34 2diahemaAún no hay calificaciones
- Spinal Cord and Tracts: Anatomy and SyndromesDocumento101 páginasSpinal Cord and Tracts: Anatomy and SyndromesZito AmoraAún no hay calificaciones
- LAPORAN KEGIATAN IGD DAN IBS BAGIAN BEDAH RSUD DR. MOEWARDI 8-14 FEBRUARI 2019Documento59 páginasLAPORAN KEGIATAN IGD DAN IBS BAGIAN BEDAH RSUD DR. MOEWARDI 8-14 FEBRUARI 2019bagus arisAún no hay calificaciones
- Pelvic Tilting and Rotations: Made by DR, Tariq Ahmad PT DPT, MSPTDocumento24 páginasPelvic Tilting and Rotations: Made by DR, Tariq Ahmad PT DPT, MSPTtariq ahmad100% (1)
- OMM One LinersDocumento21 páginasOMM One LinersBrooklyn Boo-urns100% (1)
- Orthopedics Made EasyDocumento969 páginasOrthopedics Made EasyFaraz khanAún no hay calificaciones
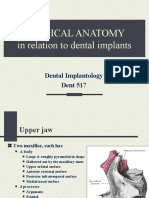
- Anatomy in Dental ImplantologyDocumento29 páginasAnatomy in Dental ImplantologyZiad RabieAún no hay calificaciones
- HUMAN BIOmuscles Origin Insertion ActionDocumento3 páginasHUMAN BIOmuscles Origin Insertion ActionandrealohrAún no hay calificaciones
- Kanghui Implant E-Catalog 2021Documento18 páginasKanghui Implant E-Catalog 2021nandagemaAún no hay calificaciones
- Nama Otot Origo Insersi Act Pectoralis MajorDocumento8 páginasNama Otot Origo Insersi Act Pectoralis MajorWilliam Giovanni M, dr.Aún no hay calificaciones
- Biomechanics & Pathomechanics of HandDocumento81 páginasBiomechanics & Pathomechanics of HandAmrita L. Tomar67% (3)
- Cartilage: Histology Dr. BernalDocumento4 páginasCartilage: Histology Dr. BernalA18- Jessa Mae DayagAún no hay calificaciones
- WORKSHEET 11 1 Locomotion and SupportDocumento7 páginasWORKSHEET 11 1 Locomotion and Supportveronica francisAún no hay calificaciones
- Leg Weakness PDFDocumento8 páginasLeg Weakness PDFamamùra maamarAún no hay calificaciones