También podría gustarte
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Republic Act No. 9173Documento11 páginasRepublic Act No. 9173Jenny SorianoAún no hay calificaciones
- Polycythemia Vera: DR - Karthik.S Moderator:Dr - Sumedh ShettyDocumento51 páginasPolycythemia Vera: DR - Karthik.S Moderator:Dr - Sumedh ShettyDr. Apoorva KottaryAún no hay calificaciones
- KONSULTA 073123 v1Documento124 páginasKONSULTA 073123 v1Substationsix MalaboncpsAún no hay calificaciones
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocumento7 páginasNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedAún no hay calificaciones
- Egypt Cochlear PresentationDocumento30 páginasEgypt Cochlear PresentationAhmad Salahuddien100% (1)
- 17 Gambling Treatment Plan2Documento3 páginas17 Gambling Treatment Plan2Navarro CaroAún no hay calificaciones
- 19-26 Faktor Risiko Kejadian Hipertensi Pada Wanita Usia Subur Di Wilayah Kerja Puskemas NaibonatDocumento8 páginas19-26 Faktor Risiko Kejadian Hipertensi Pada Wanita Usia Subur Di Wilayah Kerja Puskemas Naibonatlidya inaAún no hay calificaciones
- Acne Vulgaris A Review of Causes and Treatment.6Documento10 páginasAcne Vulgaris A Review of Causes and Treatment.6Nuwaira BalochAún no hay calificaciones
- Primay Health CentresDocumento100 páginasPrimay Health CentresBirupakshya RoutAún no hay calificaciones
- 2018 Jordanian Conference BookletDocumento51 páginas2018 Jordanian Conference BookletAurelian Corneliu MoraruAún no hay calificaciones
- Company Profile Indo Medika InternationalDocumento12 páginasCompany Profile Indo Medika InternationalshavinravizaAún no hay calificaciones
- Introduction To Electronic Medical RecordsDocumento16 páginasIntroduction To Electronic Medical RecordsSaniat Obaidullah100% (1)
- Sheehan's Syndrome PathophysiologyDocumento2 páginasSheehan's Syndrome PathophysiologyirismgallAún no hay calificaciones
- Monaco Treatment Planning Enhances Departmental EfficienciesDocumento9 páginasMonaco Treatment Planning Enhances Departmental Efficienciesricky rdnAún no hay calificaciones
- Parents Consent AY 2022 2023Documento2 páginasParents Consent AY 2022 2023Jayloid AlteaAún no hay calificaciones
- Ontario - Schedule of Benefits 2021Documento970 páginasOntario - Schedule of Benefits 2021Raj LoganathanAún no hay calificaciones
- Old Age Psychiatry LectureDocumento38 páginasOld Age Psychiatry LectureMo 'Fishpondz' IsmailAún no hay calificaciones
- Escalas de EfronDocumento2 páginasEscalas de Efronkarina100% (1)
- Inspection Report - Austin Oaks HospitalDocumento10 páginasInspection Report - Austin Oaks HospitalmilesmoffeitAún no hay calificaciones
- II MOCK TEST Questions OnlyDocumento46 páginasII MOCK TEST Questions OnlyazitaaaaaAún no hay calificaciones
- Pediatric Nur Pediatric Nur Pediatric Nur Pediatric Nur Pediatric Nursing Sing Sing Sing SingDocumento10 páginasPediatric Nur Pediatric Nur Pediatric Nur Pediatric Nur Pediatric Nursing Sing Sing Sing Singtheiam772Aún no hay calificaciones
- GiovanniDocumento6 páginasGiovanniaryaa20200% (1)
- M104 - ExamDocumento8 páginasM104 - ExamChrystal Anne Flores CorderoAún no hay calificaciones
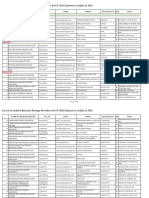
- Specimen Referral Networks FinalDocumento132 páginasSpecimen Referral Networks FinalMigori ArtAún no hay calificaciones
- Tupoksi & Indikator TO PMDT Prov - Sultra TW3Documento192 páginasTupoksi & Indikator TO PMDT Prov - Sultra TW3AryoWibowoAún no hay calificaciones
- Hypersensitivity 2Documento3 páginasHypersensitivity 2kuldip.biotechAún no hay calificaciones
- Reporte 2020 de La Oficina de Asuntos Globales de Estados UnidosDocumento72 páginasReporte 2020 de La Oficina de Asuntos Globales de Estados UnidosAristegui NoticiasAún no hay calificaciones
- 1 PBDocumento11 páginas1 PBNaswa Alifia PutriAún no hay calificaciones
- Mann Assessment of Swallowing AbilityDocumento9 páginasMann Assessment of Swallowing Abilityluca bastianiAún no hay calificaciones
- Prevenção de Trauma Perineal Revisão Cochranne 2017Documento89 páginasPrevenção de Trauma Perineal Revisão Cochranne 2017Francine XavierAún no hay calificaciones