También podría gustarte
- CVS ExaminationDocumento72 páginasCVS ExaminationPrashanthBhatAún no hay calificaciones
- Acute Abdominal PainDocumento11 páginasAcute Abdominal Painone_2_nv100% (1)
- Ekg FastlaneDocumento10 páginasEkg FastlaneAida UzunovicAún no hay calificaciones
- Shock: Not Enough Blood Flow?Documento3 páginasShock: Not Enough Blood Flow?Genevie GabrielAún no hay calificaciones
- A 34 Year Old Lady With AsthmaDocumento8 páginasA 34 Year Old Lady With AsthmaOktasi Stella NabighahAún no hay calificaciones
- Jugular Venous Pulse: Madras Medical MissionDocumento53 páginasJugular Venous Pulse: Madras Medical MissionJoshua JayakaranAún no hay calificaciones
- Assessment of The Cardiovascular SystemDocumento48 páginasAssessment of The Cardiovascular Systemkimberlyrwarren8817Aún no hay calificaciones
- Scavenger Hunt-AnswersDocumento2 páginasScavenger Hunt-Answersapi-236445988Aún no hay calificaciones
- Disorders of The BoneDocumento2 páginasDisorders of The BoneRPh Krishna Chandra JagritAún no hay calificaciones
- Acls AnpDocumento20 páginasAcls AnpNirupama KsAún no hay calificaciones
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDe EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsAún no hay calificaciones
- Pathophysiology of TuberculosisDocumento3 páginasPathophysiology of TuberculosisFirenze Fil96% (56)
- Medical Diagnosis PDFDocumento30 páginasMedical Diagnosis PDF99nonameAún no hay calificaciones
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAún no hay calificaciones
- Cardiovascular System Diseases Part 2Documento9 páginasCardiovascular System Diseases Part 2Prince Rener Velasco PeraAún no hay calificaciones
- Exercises For Stroke VictimsDocumento27 páginasExercises For Stroke VictimsProff AhengAún no hay calificaciones
- CPRDocumento9 páginasCPRMargeline PepinoAún no hay calificaciones
- Cardiac Pacing: Terms You Will Become Familiar With in This Section of TheDocumento21 páginasCardiac Pacing: Terms You Will Become Familiar With in This Section of TheClt Miskeen100% (1)
- ACLS Algorithms (2011)Documento6 páginasACLS Algorithms (2011)senbonsakuraAún no hay calificaciones
- HO - Burns Environmental EmergenciesDocumento7 páginasHO - Burns Environmental EmergenciesSteven Paul DaclesAún no hay calificaciones
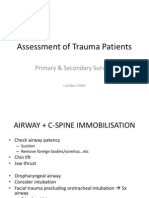
- Primary SurveyDocumento19 páginasPrimary SurveyCaroline ChauAún no hay calificaciones
- The Physiology of ShockDocumento37 páginasThe Physiology of ShockGauxy AromboAún no hay calificaciones
- ARRHYTHMIADocumento82 páginasARRHYTHMIAjiluAún no hay calificaciones
- Burn ManagementDocumento64 páginasBurn Managementabdullah100% (1)
- Sut Ams Medical College, TVMDocumento7 páginasSut Ams Medical College, TVMDIVYA R.S100% (1)
- What Is Respiratory Alkalosis?Documento3 páginasWhat Is Respiratory Alkalosis?Lorenn AdarnaAún no hay calificaciones
- Airway ManagementDocumento13 páginasAirway ManagementAlaa DaoudAún no hay calificaciones
- Financial Policy and Procedure Manual TemplateDocumento31 páginasFinancial Policy and Procedure Manual TemplatevanausabAún no hay calificaciones
- Episode 86 - HyperkalemiaDocumento7 páginasEpisode 86 - HyperkalemiaAlok yadav100% (1)
- Cardiac Meds To MemorizeDocumento4 páginasCardiac Meds To MemorizekellyaeAún no hay calificaciones
- Poisoning & BitesDocumento12 páginasPoisoning & BitesJudy HandlyAún no hay calificaciones
- Copar ExamDocumento1 páginaCopar ExamRed JimenoAún no hay calificaciones
- Nursing AssesmentDocumento39 páginasNursing AssesmentRed Jimeno100% (1)
- NEIL Trauma AssessmentDocumento3 páginasNEIL Trauma AssessmentNeil BrunoAún no hay calificaciones
- Excuse LetterDocumento1 páginaExcuse LetterRed Jimeno100% (1)
- OP PoisoningDocumento14 páginasOP PoisoningAnmol KudalAún no hay calificaciones
- ET Tube Care, Tracheostomy CareDocumento24 páginasET Tube Care, Tracheostomy CaretelilingAún no hay calificaciones
- 10 Steps To Learn ECG InterpretationDocumento5 páginas10 Steps To Learn ECG InterpretationIbrahem Y. NajjarAún no hay calificaciones
- Anterior Pituitary Gland: Fawwaz Ammari Laith & HaniDocumento22 páginasAnterior Pituitary Gland: Fawwaz Ammari Laith & HaniRashed ShatnawiAún no hay calificaciones
- Buerger'S Disease: By: Ns. Yulia Prodi S1 Keperawatan Stikes Kepanjen 2014Documento18 páginasBuerger'S Disease: By: Ns. Yulia Prodi S1 Keperawatan Stikes Kepanjen 2014atik mayasariAún no hay calificaciones
- Chest TraumaDocumento1 páginaChest TraumaelaAún no hay calificaciones
- 04 - Soft Tissue InjuriesDocumento13 páginas04 - Soft Tissue InjuriesCielo GriñoAún no hay calificaciones
- 101 Things We Should Teach Every New EMT 1) You..Documento6 páginas101 Things We Should Teach Every New EMT 1) You..Victoriano MendezAún no hay calificaciones
- EMS - Chapter 1 (Intro To EMT)Documento2 páginasEMS - Chapter 1 (Intro To EMT)Daniel Kipnis0% (1)
- AsphyxiaDocumento35 páginasAsphyxiaAna Cristina Montillano100% (1)
- Arterial Blood Gas Workshop Dr. Lanzona 12.06.07: Lala 3C-Med-09 1Documento4 páginasArterial Blood Gas Workshop Dr. Lanzona 12.06.07: Lala 3C-Med-09 1pramastutiAún no hay calificaciones
- Preventing The Spread of Bloodborne Pathogens Fact and Skill SheetsDocumento3 páginasPreventing The Spread of Bloodborne Pathogens Fact and Skill SheetsJohn Alexander GallinAún no hay calificaciones
- Introduction Definition: Types of PacemakersDocumento8 páginasIntroduction Definition: Types of PacemakersPrasann RoyAún no hay calificaciones
- Care of The Hospitalized Patient With Acute Exacerbation of CopdDocumento25 páginasCare of The Hospitalized Patient With Acute Exacerbation of CopdmiallyannaAún no hay calificaciones
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocumento15 páginasPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapAún no hay calificaciones
- CPR - Cardiopulmonary ResuscitationDocumento31 páginasCPR - Cardiopulmonary ResuscitationPanji HerlambangAún no hay calificaciones
- Net BooksDocumento2 páginasNet BooksMITHUN CHATTERJEEAún no hay calificaciones
- EMTDocumento73 páginasEMTLovely Acabado TampocoAún no hay calificaciones
- Spot The Difference Worksheet ReproductionDocumento4 páginasSpot The Difference Worksheet Reproductionapi-238643412Aún no hay calificaciones
- Organophosphorus Poisoning PDFDocumento5 páginasOrganophosphorus Poisoning PDFEliuth Zamora100% (1)
- Care of Patients With Chest TubesDocumento2 páginasCare of Patients With Chest Tubesaurezea100% (1)
- Oral Station ScenarioDocumento3 páginasOral Station ScenariojrworthingtonAún no hay calificaciones
- Kano State College of Nursing and Midwifery: Cardiac ArrestDocumento4 páginasKano State College of Nursing and Midwifery: Cardiac ArrestMuhammad Daha SanusiAún no hay calificaciones
- Coronary Artery Bypass Grafting (CABG)Documento1 páginaCoronary Artery Bypass Grafting (CABG)I.m. DanielAún no hay calificaciones
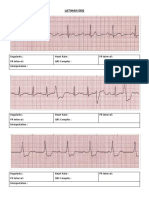
- Latihan Ekg KD A III 2016Documento15 páginasLatihan Ekg KD A III 2016Syamsul PutraAún no hay calificaciones
- BCLSDocumento25 páginasBCLSikram ullah khanAún no hay calificaciones
- Narcan and Overdoses WorksheetDocumento2 páginasNarcan and Overdoses WorksheetEmily AnnAún no hay calificaciones
- 14 Fun Facts About Your Heart: Educational VersionDe Everand14 Fun Facts About Your Heart: Educational VersionAún no hay calificaciones
- InventoryDocumento1 páginaInventoryRed JimenoAún no hay calificaciones
- Acute Coronary Syndromes AlgorithmDocumento1 páginaAcute Coronary Syndromes AlgorithmRed JimenoAún no hay calificaciones
- Company Would B Responsible ForDocumento1 páginaCompany Would B Responsible ForRed JimenoAún no hay calificaciones
- Q&A FractureDocumento13 páginasQ&A FractureRed JimenoAún no hay calificaciones
- Q&A FractureDocumento13 páginasQ&A FractureRed JimenoAún no hay calificaciones