También podría gustarte
- I. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordDocumento2 páginasI. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordERWINAún no hay calificaciones
- Obstetric Assessment ToolDocumento5 páginasObstetric Assessment ToolDudil GoatAún no hay calificaciones
- Downtime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimeDocumento5 páginasDowntime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimerupaliAún no hay calificaciones
- Nursing Assessment Form: A. Demographic DataDocumento5 páginasNursing Assessment Form: A. Demographic Datacat_w0m4nAún no hay calificaciones
- WARDWORK TemplateDocumento9 páginasWARDWORK TemplateColeen NeyraAún no hay calificaciones
- Nursing Administration AssessmentDocumento6 páginasNursing Administration Assessmentkatnebrija89Aún no hay calificaciones
- The COAT & Review Approach: How to recognise and manage unwell patientsDe EverandThe COAT & Review Approach: How to recognise and manage unwell patientsCalificación: 5 de 5 estrellas5/5 (1)
- Nursing Admission AssessmentDocumento5 páginasNursing Admission AssessmentJo MaldonadoAún no hay calificaciones
- Operating Room Nurse Interview QuestionsDocumento2 páginasOperating Room Nurse Interview Questionsali aliAún no hay calificaciones
- Gordon S Functional Health Pattern Assessment ToolDocumento10 páginasGordon S Functional Health Pattern Assessment ToolMiguel VicenteAún no hay calificaciones
- Nursing Dummy ChartDocumento4 páginasNursing Dummy Chartis_aradanasAún no hay calificaciones
- Location at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Documento5 páginasLocation at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Eduard RiparipAún no hay calificaciones
- Preoperative ChecklistDocumento1 páginaPreoperative ChecklistRyrey Abraham PacamanaAún no hay calificaciones
- Code Blue EvaluationDocumento1 páginaCode Blue EvaluationJessica Garlets0% (1)
- Pre Op ChecklistDocumento1 páginaPre Op ChecklistKoushik Reddy PodduturiAún no hay calificaciones
- Marty's Report FormDocumento1 páginaMarty's Report FormmartydailyAún no hay calificaciones
- TB QuestionnaireDocumento1 páginaTB QuestionnaireaplesgjskAún no hay calificaciones
- DAILY ROUND Head NurseDocumento1 páginaDAILY ROUND Head NurseRao Rizwan ShakoorAún no hay calificaciones
- Recovery Room Transfer SheetDocumento1 páginaRecovery Room Transfer SheetDr. Sumit Kumbhar0% (1)
- Vital Signs and Early Warning ScoresDocumento47 páginasVital Signs and Early Warning Scoresdr_nadheem100% (1)
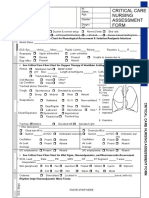
- Critical Care Nursing Assessment Form: R R R R R R R RDocumento2 páginasCritical Care Nursing Assessment Form: R R R R R R R RPipit Permata100% (1)
- Gordons Case Pres 1Documento5 páginasGordons Case Pres 1JM Asentista0% (1)
- PATIENT PRE-OPERATIVE CHECKLISTDocumento1 páginaPATIENT PRE-OPERATIVE CHECKLISTАндрій ДанильцівAún no hay calificaciones
- Emergency Department Orientation for New NursesDocumento38 páginasEmergency Department Orientation for New NursesNers SenAún no hay calificaciones
- Assigned on Admission, Transfer, and Discharge ProceduresDocumento12 páginasAssigned on Admission, Transfer, and Discharge ProceduresNagulan Nagul100% (1)
- PERIOPERATIVE NURSING PHASESDocumento11 páginasPERIOPERATIVE NURSING PHASESDa BondadAún no hay calificaciones
- IABP Learning PackageDocumento35 páginasIABP Learning PackageMuhammad Mahbøøb SadiqAún no hay calificaciones
- Heart and Neck AssessmentDocumento3 páginasHeart and Neck AssessmentKiara Ash BeethovenAún no hay calificaciones
- Mortuary Services Checklist - Random 202335531Documento4 páginasMortuary Services Checklist - Random 202335531Marion KonesAún no hay calificaciones
- Drug study patient reportDocumento1 páginaDrug study patient reportJulia Shane BarriosAún no hay calificaciones
- Integrated Cath Lab Safety ChecklistDocumento2 páginasIntegrated Cath Lab Safety ChecklistwenhalAún no hay calificaciones
- A&E Triage SystemDocumento5 páginasA&E Triage SystemArnel AlmutiahAún no hay calificaciones
- 05 Nursing Note SampleDocumento3 páginas05 Nursing Note Sampletesttest testAún no hay calificaciones
- Patient A KARDEX 1Documento2 páginasPatient A KARDEX 1Franz Patrick Legria, CPAC - SNAún no hay calificaciones
- Deficiency of Case SheetDocumento15 páginasDeficiency of Case SheetberliyaAún no hay calificaciones
- Who Safe Surgery Checklist: Sign inDocumento3 páginasWho Safe Surgery Checklist: Sign inJann Marie IsidroAún no hay calificaciones
- Push 3Documento2 páginasPush 3Sandeep SharmaAún no hay calificaciones
- Idoc - Pub - Critical Care Nursing Assessment FormDocumento3 páginasIdoc - Pub - Critical Care Nursing Assessment FormNamra AnsariAún no hay calificaciones
- SupervisorsDocumento1 páginaSupervisorsBOOKREADER_NOW100% (2)
- Outline Perioperative NursingDocumento8 páginasOutline Perioperative NursingMM VAún no hay calificaciones
- Preprocedure Check-In Sign-In Time-Out Sign-OutDocumento2 páginasPreprocedure Check-In Sign-In Time-Out Sign-OutSyahri DzikriAún no hay calificaciones
- Pediatric Assesment FormDocumento6 páginasPediatric Assesment FormJenAún no hay calificaciones
- Patient Admission Assessment FormDocumento1 páginaPatient Admission Assessment Formprasanna_326avanthiAún no hay calificaciones
- Pain Audit ToolsDocumento10 páginasPain Audit ToolsIrmela CoricAún no hay calificaciones
- Head To Toe Assessment - BRIEFDocumento2 páginasHead To Toe Assessment - BRIEFmahmoud alghaberiAún no hay calificaciones
- Student Worksheet2023 PDFDocumento2 páginasStudent Worksheet2023 PDFjj100% (1)
- Physical Examination Health AssessmentDocumento2 páginasPhysical Examination Health AssessmentRosa Willis0% (1)
- Continuous Renal Replacement Therapy (CRRT) Initial Competency Assessment and ValidationDocumento2 páginasContinuous Renal Replacement Therapy (CRRT) Initial Competency Assessment and Validationalex100% (1)
- Adult Assessment Tool 2014Documento8 páginasAdult Assessment Tool 2014Charm PradoAún no hay calificaciones
- Operating Room NotesDocumento35 páginasOperating Room NotesMagdaraog Gabrielle A.Aún no hay calificaciones
- Patient Safety and Quality ManualDocumento30 páginasPatient Safety and Quality ManualSooraj ThomasAún no hay calificaciones
- Shift Change ReportDocumento30 páginasShift Change ReportAlfi Nur Hanifah100% (1)
- 7-Performance MeasurementDocumento2 páginas7-Performance MeasurementHammad Awan100% (1)
- IWU Nursing Care Plan for 81-Year-Old Female with CHF and PneumoniaDocumento6 páginasIWU Nursing Care Plan for 81-Year-Old Female with CHF and PneumoniaclarimerAún no hay calificaciones
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDe EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsAún no hay calificaciones
- Handbook for Cssd Technicians: Understanding the Basics - Second EditionDe EverandHandbook for Cssd Technicians: Understanding the Basics - Second EditionAún no hay calificaciones
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsDe EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsAún no hay calificaciones
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersDe EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersAún no hay calificaciones
- Management of Tuberculosis: A guide for clinicians (eBook edition)De EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Aún no hay calificaciones
- IDCAP Fact SheetDocumento2 páginasIDCAP Fact SheetIDCAP2011Aún no hay calificaciones
- IDCAP Fact SheetDocumento2 páginasIDCAP Fact SheetIDCAP2011Aún no hay calificaciones
- IDCAPDocumento1 páginaIDCAPIDCAP2011Aún no hay calificaciones
- ASTMH HMIS UgandaDocumento1 páginaASTMH HMIS UgandaIDCAP2011Aún no hay calificaciones
- On-Site Support Participation by Rural Mid-Level Health Practitioners in UgandaDocumento1 páginaOn-Site Support Participation by Rural Mid-Level Health Practitioners in UgandaIDCAP2011Aún no hay calificaciones
- Computerized Health Facility Outpatient Visit FormDocumento1 páginaComputerized Health Facility Outpatient Visit FormIDCAP2011Aún no hay calificaciones
- Impact of OSS On Malaria Management 2011Documento1 páginaImpact of OSS On Malaria Management 2011IDCAP2011Aún no hay calificaciones
- Improving Outpatient Health Management Systems in UgandaDocumento1 páginaImproving Outpatient Health Management Systems in UgandaIDCAP2011Aún no hay calificaciones
- Case Scenario Final Presentation Montreal GHC 2011Documento8 páginasCase Scenario Final Presentation Montreal GHC 2011IDCAP2011Aún no hay calificaciones
- Improving Human Resources Capacity Through Evidence-Based TrainingDocumento14 páginasImproving Human Resources Capacity Through Evidence-Based TrainingIDCAP2011Aún no hay calificaciones
- Innovation in Impact EvaluationDocumento13 páginasInnovation in Impact EvaluationIDCAP2011Aún no hay calificaciones
- Advances in Medical EducationDocumento1 páginaAdvances in Medical EducationIDCAP2011Aún no hay calificaciones
- Mid-Level Practitioners' Role in Managing Infectious Diseases and Site LeadershipDocumento10 páginasMid-Level Practitioners' Role in Managing Infectious Diseases and Site LeadershipIDCAP2011Aún no hay calificaciones
- 54th ECSA Health Ministers' Conference Mombasa, KenyaDocumento29 páginas54th ECSA Health Ministers' Conference Mombasa, KenyaIDCAP2011Aún no hay calificaciones
- Clinical Performance of Mid-Level Health PractionersDocumento1 páginaClinical Performance of Mid-Level Health PractionersIDCAP2011Aún no hay calificaciones
- IDCAP ResourcesDocumento1 páginaIDCAP ResourcesIDCAP2011Aún no hay calificaciones
- IDCAP Mobile TeamsDocumento2 páginasIDCAP Mobile TeamsIDCAP2011Aún no hay calificaciones
- IDCAP Data Surveillance SystemDocumento5 páginasIDCAP Data Surveillance SystemIDCAP2011Aún no hay calificaciones
- IDCAP Bibliography (As of November 1, 2011) : Lancet. 2009 374 (9687) : 393-403Documento10 páginasIDCAP Bibliography (As of November 1, 2011) : Lancet. 2009 374 (9687) : 393-403IDCAP2011Aún no hay calificaciones
- IDCAP Bibliography (As of November 1, 2011) : Lancet. 2009 374 (9687) : 393-403Documento10 páginasIDCAP Bibliography (As of November 1, 2011) : Lancet. 2009 374 (9687) : 393-403IDCAP2011Aún no hay calificaciones
- Integrated Management of Infectious Disease (IMID)Documento3 páginasIntegrated Management of Infectious Disease (IMID)IDCAP2011Aún no hay calificaciones
- On-Site SupportDocumento2 páginasOn-Site SupportIDCAP2011Aún no hay calificaciones
- Sample Case ScenarioDocumento6 páginasSample Case ScenarioIDCAP2011Aún no hay calificaciones
- Tween 80Documento11 páginasTween 80fvdxrgAún no hay calificaciones
- Orrick PostedbyrequestDocumento4 páginasOrrick PostedbyrequestmungagungadinAún no hay calificaciones
- 100kw TSP Agenitor-404b Biogas 60-hz 480v En-827879Documento9 páginas100kw TSP Agenitor-404b Biogas 60-hz 480v En-827879Julian BarreraAún no hay calificaciones
- L4004N - 0920 - Nilfisk - Robotic-brochure-Liberty SC60Documento12 páginasL4004N - 0920 - Nilfisk - Robotic-brochure-Liberty SC60Lucianderson Marques FerreiraAún no hay calificaciones
- Unit explores Christian morality and conscienceDocumento1 páginaUnit explores Christian morality and conscienceRose Angela Mislang Uligan100% (1)
- 1 s2.0 S2214860417301148 Main PDFDocumento16 páginas1 s2.0 S2214860417301148 Main PDFQuy Hoang KimAún no hay calificaciones
- GSM Based Power Grid Monitoring SystemDocumento41 páginasGSM Based Power Grid Monitoring SystemPreetham SurepallyAún no hay calificaciones
- Class 10 Trigonometry and Application of TrigonometryDocumento1 páginaClass 10 Trigonometry and Application of TrigonometryTanmay SanchetiAún no hay calificaciones
- Self-Balancing Two-Wheeler Using GyroscopeDocumento33 páginasSelf-Balancing Two-Wheeler Using Gyroscopemilan mottaAún no hay calificaciones
- 2009 ESC Guidelines On EndocarditisDocumento45 páginas2009 ESC Guidelines On EndocarditisDaondy Friarsa SoehartoAún no hay calificaciones
- Lab 1 Free Fall GEC - CEA21 - OERSTEDDocumento6 páginasLab 1 Free Fall GEC - CEA21 - OERSTEDLee-Ann LimAún no hay calificaciones
- Diesel HatchbackDocumento14 páginasDiesel HatchbackloganathprasannaAún no hay calificaciones
- M10 - Partial Replacement of Fine Aggregate Using Polystyrene in Lightweight CHB-CE-503Documento19 páginasM10 - Partial Replacement of Fine Aggregate Using Polystyrene in Lightweight CHB-CE-503Michelle LeeAún no hay calificaciones
- Tramadol Drug StudyDocumento1 páginaTramadol Drug Studymilkv82% (11)
- DG350 ManualDocumento17 páginasDG350 ManualCareergamingAún no hay calificaciones
- Guide to Conducting SAFOP StudiesDocumento52 páginasGuide to Conducting SAFOP Studiesokemma79% (14)
- ASSEMBLING COMPUTER: HOW TO BUILD A PCDocumento48 páginasASSEMBLING COMPUTER: HOW TO BUILD A PCCeejaay PelinaAún no hay calificaciones
- 89HPES24T3G2 Hardware Design Guide: NotesDocumento10 páginas89HPES24T3G2 Hardware Design Guide: NotesDavidAún no hay calificaciones
- Purification of Morphologically and Functionally Intact Human Basophils To Near HomogeneityDocumento9 páginasPurification of Morphologically and Functionally Intact Human Basophils To Near HomogeneitySinaí GutierrezAún no hay calificaciones
- Pump Characteristics ExperimentDocumento7 páginasPump Characteristics ExperimentJam JoAún no hay calificaciones
- Journal of Alloys and Compounds: Wei Li, Zhijun Xu, Ruiqing Chu, Peng Fu, Guozhong ZangDocumento4 páginasJournal of Alloys and Compounds: Wei Li, Zhijun Xu, Ruiqing Chu, Peng Fu, Guozhong ZangSamah SamahAún no hay calificaciones
- Nutrition Effects of VitaminsDocumento21 páginasNutrition Effects of Vitaminsblessed cccAún no hay calificaciones
- Ringing On A Transmission LineDocumento33 páginasRinging On A Transmission LinePrem BhaskaraAún no hay calificaciones
- 1 SM PDFDocumento14 páginas1 SM PDFSiti HamsyiahAún no hay calificaciones
- Quant One Analyser – endless possibilitiesDocumento6 páginasQuant One Analyser – endless possibilitiesSamuel SuAún no hay calificaciones
- Classified Advertisements from Gulf Times NewspaperDocumento6 páginasClassified Advertisements from Gulf Times NewspaperAli Naveed FarookiAún no hay calificaciones
- @MedicalBooksStore 2016 AntibioticDocumento349 páginas@MedicalBooksStore 2016 Antibioticant bee100% (1)
- S10 Electric Power PackDocumento12 páginasS10 Electric Power PackrolandAún no hay calificaciones
- M. Valerio Assignment 6.1Documento1 páginaM. Valerio Assignment 6.1Mark Kristian ValerioAún no hay calificaciones
- Shop Math PDFDocumento29 páginasShop Math PDFKen LeeAún no hay calificaciones