También podría gustarte
- Bacteriology DemonstrationsDocumento12 páginasBacteriology Demonstrationshamody662002100% (1)
- Parasitology-Lec 12 TrypanosomesDocumento6 páginasParasitology-Lec 12 Trypanosomesapi-3743217Aún no hay calificaciones
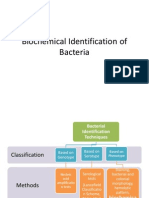
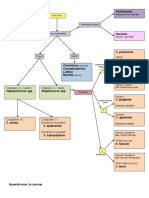
- Biochemical Identification of BacteriaDocumento72 páginasBiochemical Identification of BacteriaMaria Jhoyce MagpantayAún no hay calificaciones
- University of The Immaculate Conception: ProteinDocumento13 páginasUniversity of The Immaculate Conception: ProteinDams ZainalAún no hay calificaciones
- Biochemical Tests For Staph-Strep - OutputDocumento5 páginasBiochemical Tests For Staph-Strep - OutputJoshua Ty CayetanoAún no hay calificaciones
- Microbio Lab 8Documento4 páginasMicrobio Lab 8api-3743217100% (5)
- Parasitology-Lec 12 TrypanosomesDocumento6 páginasParasitology-Lec 12 Trypanosomesapi-3743217Aún no hay calificaciones
- Bacterial Skin and Soft Tissue InfectionsDocumento5 páginasBacterial Skin and Soft Tissue InfectionsFarid Gusranda100% (2)
- A. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusDocumento8 páginasA. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusRuel MaddawinAún no hay calificaciones
- Biochemical TestsDocumento2 páginasBiochemical TestsVishnu Reddy Vardhan PulimiAún no hay calificaciones
- Microbio Lec 5 - StreptococcusDocumento6 páginasMicrobio Lec 5 - Streptococcusapi-3743217100% (4)
- Biochemical TestsDocumento1 páginaBiochemical TestsanandnanduAún no hay calificaciones
- Gram +ve BacteriaDocumento58 páginasGram +ve BacteriaGx NavinAún no hay calificaciones
- BacteriologyDocumento11 páginasBacteriologyCarmelle Zia Reyes100% (1)
- (Microbio) Enterobacteriaceae-Dr. Natividad (Mulan)Documento11 páginas(Microbio) Enterobacteriaceae-Dr. Natividad (Mulan)Lee Delos Santos100% (3)
- (Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Documento16 páginas(Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Lee Delos Santos100% (1)
- Microbio Lec 1 - Bacterial Morphology and Ultra StructureDocumento8 páginasMicrobio Lec 1 - Bacterial Morphology and Ultra Structureapi-3743217100% (3)
- Micro ExamDocumento7 páginasMicro ExamMarie Llanes100% (1)
- Mycology and VirologyDocumento8 páginasMycology and VirologyMaybelle Acap PatnubayAún no hay calificaciones
- Microb Summary 3314Documento28 páginasMicrob Summary 3314KPAún no hay calificaciones
- Enterics Reviewer For MicrobiologyDocumento8 páginasEnterics Reviewer For MicrobiologyGea MarieAún no hay calificaciones
- Parasitology-Lec 7 Lung FlukesDocumento5 páginasParasitology-Lec 7 Lung Flukesapi-3743217100% (1)
- The Medically Important MycosesDocumento8 páginasThe Medically Important MycosesNatasha JeanAún no hay calificaciones
- Immuno Sero CompleteDocumento33 páginasImmuno Sero CompleteAngela ReyesAún no hay calificaciones
- Microbiology MnemonicsDocumento5 páginasMicrobiology MnemonicsFritzel SusbillaAún no hay calificaciones
- HistotechniquesDocumento9 páginasHistotechniquesDivineGloryMalbuyoAún no hay calificaciones
- Test Bank Exam 3Documento81 páginasTest Bank Exam 3Sajjad AhmadAún no hay calificaciones
- Microbio Lab 9,10,11,12 & ReviewDocumento3 páginasMicrobio Lab 9,10,11,12 & Reviewapi-374321750% (2)
- Clinical Microscopy: Definition and Volume Disease and Cause PolyuriaDocumento5 páginasClinical Microscopy: Definition and Volume Disease and Cause PolyuriaJovanni andesAún no hay calificaciones
- Microbio Lec 11 - Ecoli, Klebsiella Proteus, Citrobacter AnDocumento3 páginasMicrobio Lec 11 - Ecoli, Klebsiella Proteus, Citrobacter Anapi-374321750% (2)
- Clinical Bacteriology ReviewerDocumento17 páginasClinical Bacteriology Reviewer99noname100% (1)
- Gram Negative Cocci (Lecture Notes)Documento5 páginasGram Negative Cocci (Lecture Notes)Dayledaniel Sorveto100% (1)
- Triple Sugar Iron AgarDocumento9 páginasTriple Sugar Iron AgarSt HadijahAún no hay calificaciones
- Staphylococcus Spp. Gram Positive. ClusteredDocumento15 páginasStaphylococcus Spp. Gram Positive. ClusteredIvy NAún no hay calificaciones
- Bacteriology Bacterial Classification:: Sequencing Produced by The BodyDocumento2 páginasBacteriology Bacterial Classification:: Sequencing Produced by The BodyMariel TagazaAún no hay calificaciones
- Antimicrobial Susceptibility TestDocumento4 páginasAntimicrobial Susceptibility TestMATTHEW EARL MALUMAY100% (1)
- BACTERIOLOGY RecallsDocumento6 páginasBACTERIOLOGY RecallsRachelle AbonalesAún no hay calificaciones
- 3 SEMR421 Bacteriology Part 3Documento14 páginas3 SEMR421 Bacteriology Part 3Micah Daniel TapiaAún no hay calificaciones
- CC 2 Lec-CompreDocumento105 páginasCC 2 Lec-CompreLyra Dennise Llido100% (2)
- StreptococcusDocumento6 páginasStreptococcusAyessa VillacorteAún no hay calificaciones
- HashbrownDocumento22 páginasHashbrownLeomill MendiolaAún no hay calificaciones
- BacteriologyDocumento1 páginaBacteriologyCaryn RobertsonAún no hay calificaciones
- Microbiology FlashcardsDocumento36 páginasMicrobiology FlashcardsKrisha Bernadette TillamanAún no hay calificaciones
- S. Aureus: Bacteriology G Virulence Factors Clinical Diseases Treatment Staphylococcus +Documento4 páginasS. Aureus: Bacteriology G Virulence Factors Clinical Diseases Treatment Staphylococcus +MARIA FREDIJEAN CARIÑOAún no hay calificaciones
- Chapter 2 Introduction To Urinalysis PDFDocumento4 páginasChapter 2 Introduction To Urinalysis PDFJulie Anne Soro ValdezAún no hay calificaciones
- MycoViro 2Documento44 páginasMycoViro 2Ria AlcantaraAún no hay calificaciones
- Clinical MicrosDocumento28 páginasClinical MicrosKristine Jamella Maris NaragAún no hay calificaciones
- Christian Villahermosa March 4, 2021: Philippine HIV and AIDS Policy ActDocumento14 páginasChristian Villahermosa March 4, 2021: Philippine HIV and AIDS Policy ActvenusAún no hay calificaciones
- Staphylococci: Streptococcus PyogenesDocumento20 páginasStaphylococci: Streptococcus PyogenesPharmacy2015100% (2)
- Gram Staining 01Documento11 páginasGram Staining 01MARICAR RAFAELAún no hay calificaciones
- Virology Notes (RNA Virus)Documento2 páginasVirology Notes (RNA Virus)Mary Christelle100% (1)
- Serological TestsDocumento2 páginasSerological TestsKimberly EspaldonAún no hay calificaciones
- Summary of Diagnostic BacteriologyDocumento45 páginasSummary of Diagnostic Bacteriologyomaromran100% (3)
- MicrobiologyDocumento49 páginasMicrobiologyinnyAún no hay calificaciones
- Gram Negative RodsDocumento8 páginasGram Negative RodsRuel Maddawin100% (1)
- Chemical ExaminationDocumento42 páginasChemical ExaminationLAb Meh100% (2)
- Microbiology Memorization SheetDocumento5 páginasMicrobiology Memorization Sheetalobrien100% (1)
- Mycobacteria: Nocardia, Rhodococcus, Tsukamurella and GordoniaDocumento7 páginasMycobacteria: Nocardia, Rhodococcus, Tsukamurella and Gordonia20C – Gorospe, Rhai Chezka V.Aún no hay calificaciones
- Vibrio (Comma-Shaped or Curved Bacillus)Documento10 páginasVibrio (Comma-Shaped or Curved Bacillus)Ira ElizagaAún no hay calificaciones
- CLINICAL CHEMISTRY: Passbooks Study GuideDe EverandCLINICAL CHEMISTRY: Passbooks Study GuideAún no hay calificaciones
- Medical Technologist: Passbooks Study GuideDe EverandMedical Technologist: Passbooks Study GuideAún no hay calificaciones
- L1 - StaphylococciDocumento35 páginasL1 - Staphylococciyouservezeropurpose113Aún no hay calificaciones
- The Staphylococci: Lecture SixDocumento8 páginasThe Staphylococci: Lecture SixjohnsmithprayAún no hay calificaciones
- Clin Path Lab 6 UrinalysisDocumento5 páginasClin Path Lab 6 Urinalysisapi-3743217100% (6)
- Microbio Lab 9,10,11,12 & ReviewDocumento3 páginasMicrobio Lab 9,10,11,12 & Reviewapi-374321750% (2)
- Clin Path Lab 6 Urinalysis Part 2Documento7 páginasClin Path Lab 6 Urinalysis Part 2api-3743217100% (3)
- Microbio Lec 10 - Enterobacteriaceae Gen, Shigella and SalmoDocumento8 páginasMicrobio Lec 10 - Enterobacteriaceae Gen, Shigella and Salmoapi-3743217100% (7)
- Microbio Lec 11 - Ecoli, Klebsiella Proteus, Citrobacter AnDocumento3 páginasMicrobio Lec 11 - Ecoli, Klebsiella Proteus, Citrobacter Anapi-374321750% (2)
- Microbio Lab 6Documento4 páginasMicrobio Lab 6api-374321750% (2)
- Microbio Lec 8 - MycobacteriaDocumento6 páginasMicrobio Lec 8 - Mycobacteriaapi-374321750% (2)
- Microbio Lab 7 (Leigh)Documento8 páginasMicrobio Lab 7 (Leigh)api-3743217100% (6)
- Para Lab 4Documento3 páginasPara Lab 4api-3743217Aún no hay calificaciones
- Microbio Lec 1 - Bacterial Morphology and Ultra StructureDocumento8 páginasMicrobio Lec 1 - Bacterial Morphology and Ultra Structureapi-3743217100% (3)
- Para Lab 11Documento3 páginasPara Lab 11api-3743217Aún no hay calificaciones
- Parasitology-Lec 13 MalariaDocumento6 páginasParasitology-Lec 13 Malariaapi-3743217Aún no hay calificaciones
- Para Lab 8Documento2 páginasPara Lab 8api-3743217100% (2)
- Parasitology-Lec 10 EntamoebaDocumento7 páginasParasitology-Lec 10 Entamoebaapi-3743217100% (2)
- Parasitology-Lec 9 CestodesDocumento5 páginasParasitology-Lec 9 Cestodesapi-3743217100% (4)
- Kuliah Pioderma DR Asih BudiastutiDocumento56 páginasKuliah Pioderma DR Asih BudiastutiunisoldierAún no hay calificaciones
- Ashwagandha Leaves Medicinal UsesDocumento3 páginasAshwagandha Leaves Medicinal UsesSanjay PatilAún no hay calificaciones
- Interdigital Comedones Laser SurgeryDocumento8 páginasInterdigital Comedones Laser SurgeryFHVCYLAún no hay calificaciones
- Bullous Disorders, Bacterial and Fungal Skin InfectionsDocumento95 páginasBullous Disorders, Bacterial and Fungal Skin InfectionsDeborah ChemutaiAún no hay calificaciones
- Collection of Systematic Bacteriology (Mansoura Dentistry)Documento16 páginasCollection of Systematic Bacteriology (Mansoura Dentistry)elsayed barhomeAún no hay calificaciones
- DR Angelo Smith M.D WHPLDocumento95 páginasDR Angelo Smith M.D WHPLMuhammad Riaz BhattiAún no hay calificaciones
- Kode Klasifikasi Diagnosis Dan TerminologiDocumento21 páginasKode Klasifikasi Diagnosis Dan TerminologiDini KingkinAún no hay calificaciones
- Lecture 5 MicrobiologyDocumento89 páginasLecture 5 Microbiologyjessenia.tutor2010Aún no hay calificaciones
- Surgical InfectionsDocumento55 páginasSurgical InfectionsvichramAún no hay calificaciones
- Unit 4 BacteriologyDocumento51 páginasUnit 4 BacteriologySharmila LamisharAún no hay calificaciones
- Module 3 HomeworkDocumento6 páginasModule 3 HomeworkCj LinceAún no hay calificaciones
- Salin2 PPT ProposalDocumento22 páginasSalin2 PPT ProposalSultan HSBAún no hay calificaciones
- Boils TreatmentsDocumento8 páginasBoils Treatmentsadampitt587Aún no hay calificaciones
- Microbiology Viriology and ImmunologyDocumento44 páginasMicrobiology Viriology and ImmunologyRoseline AdebisiAún no hay calificaciones
- Chapter 3 Lecture - The Integumentary System (Part 1 and Part 2 Combined)Documento25 páginasChapter 3 Lecture - The Integumentary System (Part 1 and Part 2 Combined)CARLA PADILLAAún no hay calificaciones
- Boil On Skin Reason - Google SearchDocumento1 páginaBoil On Skin Reason - Google SearchMahrukh WaseemAún no hay calificaciones
- Bacterial Infections DD3Documento38 páginasBacterial Infections DD3hhhsAún no hay calificaciones
- N11 Chan Chloe Micropara 103 Compilation of Microbial Diseases Final RequirementDocumento46 páginasN11 Chan Chloe Micropara 103 Compilation of Microbial Diseases Final RequirementCHLOE CATHERINE CHANAún no hay calificaciones
- Module 2 PPDocumento10 páginasModule 2 PPAldous FajardoAún no hay calificaciones
- Indian Journal of Homoeopathic MedicineDocumento29 páginasIndian Journal of Homoeopathic MedicineDinesh DhokeAún no hay calificaciones
- Tabel Referensi Diagnosa Non Spesialistik Baru: Kompetensi Obat Alat Laboratorium LainnyaDocumento4 páginasTabel Referensi Diagnosa Non Spesialistik Baru: Kompetensi Obat Alat Laboratorium LainnyaArmaludink KlorofilAún no hay calificaciones
- Secundum Artem: Compounding For Otic DisordersDocumento0 páginasSecundum Artem: Compounding For Otic Disordersdebieyolanda_7180456Aún no hay calificaciones
- Daftar Diagnosa Non Spesialistik Yang Bisa Ditangani TuntasDocumento9 páginasDaftar Diagnosa Non Spesialistik Yang Bisa Ditangani TuntasarieAún no hay calificaciones
- Healing PowersDocumento9 páginasHealing PowersJack Key Chan AntigAún no hay calificaciones
- AbscessDocumento4 páginasAbscessShivBalakChauhanAún no hay calificaciones
- Rife List 5000 PDFDocumento161 páginasRife List 5000 PDFAnnelie RabieAún no hay calificaciones
- Cellulitis and Skin AbscessDocumento18 páginasCellulitis and Skin AbscessAnonymous ZUaUz1wwAún no hay calificaciones
- Diagnosa Non SpesialistikDocumento12 páginasDiagnosa Non SpesialistikWahyu PedjeAún no hay calificaciones
- Saline Compresses For Radiation Skin ReactionsDocumento2 páginasSaline Compresses For Radiation Skin ReactionsVianne MaryAún no hay calificaciones