También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Edaic 3Documento16 páginasEdaic 3DsdAún no hay calificaciones
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- NeuVision 900 Operation+ManualDocumento169 páginasNeuVision 900 Operation+ManualRafael Salazar100% (1)
- Living and Dying With Medical Technology: Daniel Callahan, PHDDocumento3 páginasLiving and Dying With Medical Technology: Daniel Callahan, PHDogianneoAún no hay calificaciones
- AtelectasisDocumento9 páginasAtelectasisArni ZulsitaAún no hay calificaciones
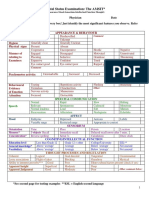
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocumento2 páginasMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- PTSD Treatment ManualDocumento54 páginasPTSD Treatment Manualdrjchandler100% (4)
- Ladewig 8e TIF Ch01 PDFDocumento13 páginasLadewig 8e TIF Ch01 PDFjames smithAún no hay calificaciones
- Respironics V60 Users Manual PDFDocumento160 páginasRespironics V60 Users Manual PDFEduardoAún no hay calificaciones
- THE HR Chronicle - November'19Documento8 páginasTHE HR Chronicle - November'19DrSwati Jayant PawarAún no hay calificaciones
- Assessment of MalingeringDocumento12 páginasAssessment of MalingeringkosmicAún no hay calificaciones
- Nurse ResumeDocumento1 páginaNurse Resumeapi-400113721Aún no hay calificaciones
- Speech Language Pathology: Background and NatureDocumento8 páginasSpeech Language Pathology: Background and NatureNikki Nina Arabe BarcinasAún no hay calificaciones
- AOTA Adaptation To Macular Escotomas in Persons With Low VisionDocumento7 páginasAOTA Adaptation To Macular Escotomas in Persons With Low VisionadelitaperezAún no hay calificaciones
- Tongue in Complete DentureDocumento8 páginasTongue in Complete DentureAman SachdevaAún no hay calificaciones
- Salient Features - MPPRC DIARRHEA RevisedDocumento12 páginasSalient Features - MPPRC DIARRHEA RevisedLui Yalong Jr.Aún no hay calificaciones
- Advanced Level - ReadingDocumento5 páginasAdvanced Level - ReadingLarry SmithAún no hay calificaciones
- Shëndeti Mendor I Fëmijlve Dhe Adoleshentëve Prizren Naim FanajDocumento1 páginaShëndeti Mendor I Fëmijlve Dhe Adoleshentëve Prizren Naim Fanajlulkuqe029Aún no hay calificaciones
- Musculosceletal Block: Prof - Dr.Dr. Bambang Pardjianto, SPB., Spbp-Re (K)Documento32 páginasMusculosceletal Block: Prof - Dr.Dr. Bambang Pardjianto, SPB., Spbp-Re (K)Irsyad Robani WAún no hay calificaciones
- Referat CA PancreasDocumento25 páginasReferat CA PancreasPamela VasikhaAún no hay calificaciones
- Edoc - Pub Community Health Nursing Notes SummaryDocumento9 páginasEdoc - Pub Community Health Nursing Notes SummarySHAH BAZAún no hay calificaciones
- Kokinakos Chris ResumeDocumento1 páginaKokinakos Chris Resumeapi-375717994Aún no hay calificaciones
- MIASMS THE REAL TRACK TO CUREDocumento5 páginasMIASMS THE REAL TRACK TO CUREjiurgiuAún no hay calificaciones
- Subject: - Legal NoticeDocumento2 páginasSubject: - Legal NoticeHarmeet SinghAún no hay calificaciones
- SerologyDocumento33 páginasSerologyGEBEYAW ADDISUAún no hay calificaciones
- Neuro-Associative Conditioning: Programing Your Trading Mind'Documento21 páginasNeuro-Associative Conditioning: Programing Your Trading Mind'ediAún no hay calificaciones
- Open Bone Grafting: Papineau TechniqueDocumento7 páginasOpen Bone Grafting: Papineau TechniqueAlireza MirzasadeghiAún no hay calificaciones
- LCD PresentationDocumento38 páginasLCD PresentationAnaz HamzaAún no hay calificaciones
- Burnout Syndrome - in NursingDocumento5 páginasBurnout Syndrome - in NursingIOSRjournalAún no hay calificaciones
- Thoracic Trauma: The Deadly DozenDocumento20 páginasThoracic Trauma: The Deadly DozenPANTS1Aún no hay calificaciones
- Neurological Disorders Practice Test QuestionsDocumento6 páginasNeurological Disorders Practice Test QuestionsBenedict AlvarezAún no hay calificaciones