También podría gustarte
- Surgical InstrumentsDocumento8 páginasSurgical InstrumentsSharmaine Simon91% (11)
- Common Medical Abbreviations With MeaningsDocumento16 páginasCommon Medical Abbreviations With MeaningsWilliam Franz SyAún no hay calificaciones
- Drug Study (Ranitidine, Metoclopramide, Ketorolac, and Omeprazole)Documento8 páginasDrug Study (Ranitidine, Metoclopramide, Ketorolac, and Omeprazole)Akisan0% (1)
- 6th Central Pay Commission Salary CalculatorDocumento15 páginas6th Central Pay Commission Salary Calculatorrakhonde100% (436)
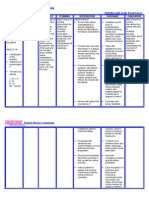
- NURSING CARE PLAN - Breast CancerDocumento2 páginasNURSING CARE PLAN - Breast Cancerderic100% (3)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Manuscript Provisional PDF: An Unusual Cause of HypertensionDocumento3 páginasManuscript Provisional PDF: An Unusual Cause of HypertensionjoelrequenaAún no hay calificaciones
- AD33 - Duck Keeping in The TropicsDocumento80 páginasAD33 - Duck Keeping in The TropicsriksanagaraAún no hay calificaciones
- Understanding The Contact Tracing Reporting TemplateDocumento51 páginasUnderstanding The Contact Tracing Reporting TemplateAlvin Lee Cucio AsuroAún no hay calificaciones
- Annual Losses Due To Mastitis Above A Desirable Baseline Level Example DairyDocumento4 páginasAnnual Losses Due To Mastitis Above A Desirable Baseline Level Example DairycapsfastAún no hay calificaciones
- Delta Green - Autopsy of A Sand DwellerDocumento2 páginasDelta Green - Autopsy of A Sand DwellerLuca LiperiAún no hay calificaciones
- Bio Immune Gas Exchange MarkschemeDocumento4 páginasBio Immune Gas Exchange Markschemeyt kAún no hay calificaciones
- Gynaecological NursingDocumento79 páginasGynaecological NursingGuruKPO100% (3)
- OSCE ChecklistDocumento13 páginasOSCE Checklistjmiller623Aún no hay calificaciones
- Glencolmcille Agricultural Show Entry Booklet 2013Documento16 páginasGlencolmcille Agricultural Show Entry Booklet 2013Glencolmcille ShowAún no hay calificaciones
- Thoracic Trauma TreatmentDocumento77 páginasThoracic Trauma TreatmentAnonymous GsvDOlQuSAún no hay calificaciones
- Chromosome Structure and FunctionDocumento76 páginasChromosome Structure and Functionstevensb055Aún no hay calificaciones
- Batuk EfektifDocumento6 páginasBatuk EfektifVia Eliadora TogatoropAún no hay calificaciones
- Another DedicationDocumento21 páginasAnother DedicationFarida AdiningrumAún no hay calificaciones
- 100 Weird Facts About The Human BodyDocumento11 páginas100 Weird Facts About The Human Bodycryonics20039984Aún no hay calificaciones
- Blood LecturesDocumento128 páginasBlood LecturessrhrenaissanceAún no hay calificaciones
- General Medicine MCQDocumento11 páginasGeneral Medicine MCQsami1218100% (3)
- Chyawanprash, a household remedy in northern IndiaDocumento5 páginasChyawanprash, a household remedy in northern IndiaA K VermaAún no hay calificaciones
- Discrepancy Index Worksheet For Print PDFDocumento1 páginaDiscrepancy Index Worksheet For Print PDFTatiAún no hay calificaciones
- A Case PresentationDocumento50 páginasA Case PresentationAnaleah MalayaoAún no hay calificaciones
- Concise Atlas of Basic HemopoiesisDocumento14 páginasConcise Atlas of Basic HemopoiesisdynndgrAún no hay calificaciones
- CCGL 9061 PosterDocumento1 páginaCCGL 9061 Posterchunpan tsangAún no hay calificaciones
- Vector-Borne Disease Management ProgrammesDocumento44 páginasVector-Borne Disease Management ProgrammesInternational Association of Oil and Gas Producers100% (1)
- Route of AdministrationDocumento10 páginasRoute of Administration言爱邦Aún no hay calificaciones
- FlapsDocumento27 páginasFlapsstegarescupavelAún no hay calificaciones
- Acid Base Balance and Arterial Blood Gas AnalysisDocumento29 páginasAcid Base Balance and Arterial Blood Gas AnalysisPaulus LukmanAún no hay calificaciones
- How Pandemics Spread and WebquestDocumento3 páginasHow Pandemics Spread and Webquestapi-405140390Aún no hay calificaciones
- The many health benefits of pet ownershipDocumento6 páginasThe many health benefits of pet ownershipNamashya SahooAún no hay calificaciones
- Plasticity and The BrainDocumento0 páginasPlasticity and The BrainscscolivesAún no hay calificaciones
- AgustusDocumento25 páginasAgustusEndah SetyowatiAún no hay calificaciones
- 20 Lecture PresentationDocumento82 páginas20 Lecture PresentationMaja Torlo100% (1)