También podría gustarte
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- E - TutoringDocumento4 páginasE - Tutoringdrkvsubramanian100% (1)
- Value Chain Analysis1Documento29 páginasValue Chain Analysis1ramyasathishAún no hay calificaciones
- Mathletics Grade 1 - Chance and DataDocumento25 páginasMathletics Grade 1 - Chance and DataMadeleine EsperanzaAún no hay calificaciones
- "Swiggy Strike": Case StudyDocumento7 páginas"Swiggy Strike": Case StudyRavi JindalAún no hay calificaciones
- Azu Etd 13902 Sip1 MDocumento301 páginasAzu Etd 13902 Sip1 Mlamaga98Aún no hay calificaciones
- Ron Kaufman - Uplifting ServiceDocumento1 páginaRon Kaufman - Uplifting ServicefmshaonAún no hay calificaciones
- Cultural Atlas - Australian Culture - Core ConceptsDocumento14 páginasCultural Atlas - Australian Culture - Core ConceptsRear BaueltazarAún no hay calificaciones
- New War Fronts Lie in Economic Zones (Essay Outline by - Awais Aftab Butt)Documento3 páginasNew War Fronts Lie in Economic Zones (Essay Outline by - Awais Aftab Butt)sajjad hussainAún no hay calificaciones
- Crowdsourcing and Social Engagement:: Potential, Power and Freedom For Libraries and UsersDocumento73 páginasCrowdsourcing and Social Engagement:: Potential, Power and Freedom For Libraries and Usersjaypee pengAún no hay calificaciones
- Jedediah Buxton - IpcnaDocumento3 páginasJedediah Buxton - IpcnaAngello TamayoAún no hay calificaciones
- Portfolio Template in Earth ScienceDocumento10 páginasPortfolio Template in Earth ScienceAngelica Olasiman EsganaAún no hay calificaciones
- Navedtra 130b Vol-IIDocumento148 páginasNavedtra 130b Vol-IIstephenhuAún no hay calificaciones
- For SouvenirDocumento1 páginaFor SouvenirKarizza Zoette Ann AlcardeAún no hay calificaciones
- Adm 551 HRM Topic 1 HRM PerspectiveDocumento39 páginasAdm 551 HRM Topic 1 HRM PerspectiveAirin SamuelAún no hay calificaciones
- 100 Workouts Vol3 PDFDocumento211 páginas100 Workouts Vol3 PDFpink lady100% (4)
- M - A - (Journalism & Mass Communication) - 309 12 - Evolution of Media PDFDocumento212 páginasM - A - (Journalism & Mass Communication) - 309 12 - Evolution of Media PDFdev rs100% (1)
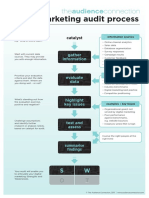
- Digital Marketing Audit Process: CatalystDocumento1 páginaDigital Marketing Audit Process: CatalysttdeviyanAún no hay calificaciones
- ObhrmDocumento30 páginasObhrmvamaAún no hay calificaciones
- Excercise - Terminal Area - JICA - Wbook 2 PDFDocumento1 páginaExcercise - Terminal Area - JICA - Wbook 2 PDFDipendra ShresthaAún no hay calificaciones
- Welcome: Sibugay Technical Institute, IncorporatedDocumento24 páginasWelcome: Sibugay Technical Institute, Incorporatedjessica navajaAún no hay calificaciones
- A.P.S C H E: Hall Ticket No. Rank: Candidate Name: Father's Name: Gender: Caste/ RegionDocumento1 páginaA.P.S C H E: Hall Ticket No. Rank: Candidate Name: Father's Name: Gender: Caste/ RegionVicky BscAún no hay calificaciones
- Health Optimizing Grade 12 P eDocumento4 páginasHealth Optimizing Grade 12 P eKookie100% (1)
- Imperial College London Graduation Ceremony Terms and Conditions 2019Documento9 páginasImperial College London Graduation Ceremony Terms and Conditions 2019Riza Agung NugrahaAún no hay calificaciones
- 2020-11-05 Calvert County TimesDocumento28 páginas2020-11-05 Calvert County TimesSouthern Maryland OnlineAún no hay calificaciones
- Penilaian AutentikDocumento6 páginasPenilaian AutentikslametAún no hay calificaciones
- JLPT N1 Vocab ListDocumento241 páginasJLPT N1 Vocab ListKennedy GitauAún no hay calificaciones
- Socio Economic Diversity and Its Effect On HRMDocumento3 páginasSocio Economic Diversity and Its Effect On HRMKim Joyce Pantanoza AlimorongAún no hay calificaciones
- SHS Contextualized Research in Daily Life 2 CGDocumento6 páginasSHS Contextualized Research in Daily Life 2 CGGerald Jem Bernandino100% (2)
- A Comparative Study of The Provisions OF ACI: 318-08 AND IS: 456-2000 BUILDING Codes For Design of Flat SlabsDocumento3 páginasA Comparative Study of The Provisions OF ACI: 318-08 AND IS: 456-2000 BUILDING Codes For Design of Flat Slabswafiullah sayedAún no hay calificaciones
- Sample Memo 1Documento20 páginasSample Memo 1Akshar JindalAún no hay calificaciones