También podría gustarte
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- 6 SbarDocumento11 páginas6 Sbarsathish kumarAún no hay calificaciones
- Laparoscopic AdrenalectomyDocumento21 páginasLaparoscopic AdrenalectomyHu EyongAún no hay calificaciones
- Blood Circulation and Transport ModuleDocumento15 páginasBlood Circulation and Transport ModuleIella's Rashid100% (1)
- The Problem of Validity in Field Studies of Psychological Disorders Revisited 1990Documento14 páginasThe Problem of Validity in Field Studies of Psychological Disorders Revisited 1990FiorellaAún no hay calificaciones
- 5th Medicine O0SCE Collection 5Documento69 páginas5th Medicine O0SCE Collection 5Yousif Fawzi Al-DilaijanAún no hay calificaciones
- What Is The Follicular Phase?: Good To KnowDocumento3 páginasWhat Is The Follicular Phase?: Good To KnowNancy SinghAún no hay calificaciones
- Hospital ListDocumento3 páginasHospital ListShoaib MalikAún no hay calificaciones
- Case 1 - Kasey KoxDocumento6 páginasCase 1 - Kasey Koxface faceAún no hay calificaciones
- Fagerstrom Test For Nicotine DependenceDocumento31 páginasFagerstrom Test For Nicotine DependenceMark OmbaoAún no hay calificaciones
- PATH - Bony Injuries (Fractures) (8p) PDFDocumento8 páginasPATH - Bony Injuries (Fractures) (8p) PDFandreeaAún no hay calificaciones
- Pediatric Inguinal Hernia PDFDocumento5 páginasPediatric Inguinal Hernia PDFade-djufrieAún no hay calificaciones
- Artificial Hip Joint/Hip Replacement: Muhammad Akmal Qaisar 08-PWMCT-0056 Mechanical Engg DesignDocumento18 páginasArtificial Hip Joint/Hip Replacement: Muhammad Akmal Qaisar 08-PWMCT-0056 Mechanical Engg DesignAkmalAún no hay calificaciones
- Osh 6301Documento4 páginasOsh 6301Hassan ShahzadAún no hay calificaciones
- Sicca Syndrome in Patients HIVDocumento6 páginasSicca Syndrome in Patients HIVkagone walidAún no hay calificaciones
- NCCN HCC For Patients 2020Documento76 páginasNCCN HCC For Patients 2020Dona LagurinAún no hay calificaciones
- [Advances in Neurosurgery 2] O. Stochdorph (Auth.), W. Klug, M. Brock, M. Klinger, O. Spoerri (Eds.) - Meningiomas Diagnostic and Therapeutic Problems Multiple Sclerosis Misdiagnosis Forensic Problems in NeurosurgDocumento461 páginas[Advances in Neurosurgery 2] O. Stochdorph (Auth.), W. Klug, M. Brock, M. Klinger, O. Spoerri (Eds.) - Meningiomas Diagnostic and Therapeutic Problems Multiple Sclerosis Misdiagnosis Forensic Problems in Neurosurgbayu_gendeng666Aún no hay calificaciones
- Growth - Development of Fetus - NeonateDocumento40 páginasGrowth - Development of Fetus - NeonatesujidahAún no hay calificaciones
- Physiotherapy Management For THR and DHSDocumento5 páginasPhysiotherapy Management For THR and DHSHaris KhanAún no hay calificaciones
- Gram Negative Rods: Oxidase TestDocumento1 páginaGram Negative Rods: Oxidase Testnaura ghinaAún no hay calificaciones
- Body Story The FluDocumento1 páginaBody Story The FlujordanAún no hay calificaciones
- Assignment in NCM 106 LectureDocumento6 páginasAssignment in NCM 106 LectureJeanessa Delantar QuilisadioAún no hay calificaciones
- Cefaleia - ContinuumDocumento195 páginasCefaleia - ContinuumRafaelAún no hay calificaciones
- B BlockersDocumento5 páginasB BlockersBo GrayAún no hay calificaciones
- Dencover ClaimformDocumento4 páginasDencover Claimformd763106Aún no hay calificaciones
- HDA 2018 Puerto Rico Mini Congress September 27-30 2018Documento2 páginasHDA 2018 Puerto Rico Mini Congress September 27-30 2018HispanicMarketAdvisorsAún no hay calificaciones
- Module 1 Am Activity On Prioritization v2Documento5 páginasModule 1 Am Activity On Prioritization v2KeanuAún no hay calificaciones
- MSDS Sysmex Hematology EIGHTCHECK-3WP - 30jun12-3Documento4 páginasMSDS Sysmex Hematology EIGHTCHECK-3WP - 30jun12-3Laboratorium RswkAún no hay calificaciones
- High Risk NeonatesDocumento58 páginasHigh Risk Neonatesskybluedugs100% (1)
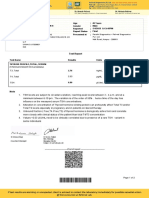
- Patient Report BALRAM SINGHDocumento2 páginasPatient Report BALRAM SINGHNeeraj KumarAún no hay calificaciones
- Herbal Medicine and The Gastrointestinal SystemDocumento79 páginasHerbal Medicine and The Gastrointestinal Systemryanti adlanAún no hay calificaciones
























































![[Advances in Neurosurgery 2] O. Stochdorph (Auth.), W. Klug, M. Brock, M. Klinger, O. Spoerri (Eds.) - Meningiomas Diagnostic and Therapeutic Problems Multiple Sclerosis Misdiagnosis Forensic Problems in Neurosurg](https://imgv2-2-f.scribdassets.com/img/document/375359245/149x198/fae4c10859/1522685798?v=1)