También podría gustarte
- Essential Endodontology PDFDocumento402 páginasEssential Endodontology PDFDiana Jeverdan100% (1)
- Comprehensive and Clinical Anatomy of the Middle EarDe EverandComprehensive and Clinical Anatomy of the Middle EarAún no hay calificaciones
- Finding Big Alpha in Big Data. The Evolution of Active Investing - 2015Documento8 páginasFinding Big Alpha in Big Data. The Evolution of Active Investing - 2015bogdimAún no hay calificaciones
- J Esthet Restor Dent - 2022 - Ferrari - Restorative Difficulty Evaluation System of Endodontically Treated TeethDocumento16 páginasJ Esthet Restor Dent - 2022 - Ferrari - Restorative Difficulty Evaluation System of Endodontically Treated TeethViridiana EliasAún no hay calificaciones
- ENDODONTICS (Ingle) PDFDocumento1022 páginasENDODONTICS (Ingle) PDFAnonymous Bt6favSF4Y78% (9)
- Endo Vs Implant SeminarDocumento25 páginasEndo Vs Implant Seminarsweetminu99100% (1)
- MCQ Edition 8 (Pathway) - Q&ADocumento57 páginasMCQ Edition 8 (Pathway) - Q&Aareej alblowiAún no hay calificaciones
- The Clinical Significance of The Retromolar Canal and Foramen in DentistryDocumento24 páginasThe Clinical Significance of The Retromolar Canal and Foramen in Dentistryمحمد عبدالرحمنAún no hay calificaciones
- No Srat 2015Documento6 páginasNo Srat 2015Gaby GuzmanAún no hay calificaciones
- Endodontic Considerations in Three-Canalled Premolars A Practical Update PDFDocumento4 páginasEndodontic Considerations in Three-Canalled Premolars A Practical Update PDFLeticia RiveraAún no hay calificaciones
- Lana JP 2011 Anatomic Variations and Lesions of The Maxillary SinusDocumento6 páginasLana JP 2011 Anatomic Variations and Lesions of The Maxillary Sinusmarlene tamayoAún no hay calificaciones
- Azim 2015Documento5 páginasAzim 2015Andrei BerdichewskyAún no hay calificaciones
- Oral CencerDocumento14 páginasOral CencerVilaseca224466Aún no hay calificaciones
- MainDocumento16 páginasMainel verdaderoAún no hay calificaciones
- Incidence of Middle Mesial Canals Based On Distance Between Mesial Canal Orifices in Mandibular Molars A Clinical and Cone-Beam Computed Tomographic AnalysisDocumento4 páginasIncidence of Middle Mesial Canals Based On Distance Between Mesial Canal Orifices in Mandibular Molars A Clinical and Cone-Beam Computed Tomographic Analysisimran khanAún no hay calificaciones
- Art. 5 Analysis of The Internal Anatomy of Maxillary First Molars by Using Different MethodsDocumento6 páginasArt. 5 Analysis of The Internal Anatomy of Maxillary First Molars by Using Different MethodsXime M.RAún no hay calificaciones
- EndoDocumento3 páginasEndoshobhana20Aún no hay calificaciones
- Missed Anatomy - Frequency and Clinical ImpactDocumento29 páginasMissed Anatomy - Frequency and Clinical ImpactFerdi gamerAún no hay calificaciones
- Conductos Medio-Mesiales en Primeros Molares Inferiores Permanentes Reporte de Tres Casos ClínicosDocumento7 páginasConductos Medio-Mesiales en Primeros Molares Inferiores Permanentes Reporte de Tres Casos ClínicosDexterAún no hay calificaciones
- 3-Dimensional Analysis and Literature Review of The Root Canal Morphology and Physiological Foramen Geometry of 125 Mandibular Incisors by Means of Micro-Computed Tomography in A German PopulationDocumento8 páginas3-Dimensional Analysis and Literature Review of The Root Canal Morphology and Physiological Foramen Geometry of 125 Mandibular Incisors by Means of Micro-Computed Tomography in A German PopulationalondraAún no hay calificaciones
- Int Endodontic J - 2014 - Ordinola Zapata - Micro CT Evaluation of C Shaped Mandibular First Premolars in A BrazilianDocumento7 páginasInt Endodontic J - 2014 - Ordinola Zapata - Micro CT Evaluation of C Shaped Mandibular First Premolars in A BrazilianRodrigo Cassana RojasAún no hay calificaciones
- Identification and Endodontic Management of Confluent Middle Mesial Canal in Mandibular First Molar A Case Report.20150306124240Documento4 páginasIdentification and Endodontic Management of Confluent Middle Mesial Canal in Mandibular First Molar A Case Report.20150306124240dini anitaAún no hay calificaciones
- Prevalence and Location of The Secondary Mesiobuccal Canal in 1,100 Maxillary Molars Using Cone Beam Computed TomographyDocumento8 páginasPrevalence and Location of The Secondary Mesiobuccal Canal in 1,100 Maxillary Molars Using Cone Beam Computed TomographySaray ValerioAún no hay calificaciones
- 2ms Con 3 RaicesDocumento5 páginas2ms Con 3 RaicesFiorella AlexandraAún no hay calificaciones
- JornalDocumento12 páginasJornalNida SaifanaAún no hay calificaciones
- Cleghorn 2006Documento8 páginasCleghorn 2006Alvaro Alarcon ValenzuelaAún no hay calificaciones
- Three Root Canals in The Mesiobuccal Root of Maxillary Molars: Case Reports and Literature ReviewDocumento8 páginasThree Root Canals in The Mesiobuccal Root of Maxillary Molars: Case Reports and Literature ReviewJing XueAún no hay calificaciones
- Clinical Article Canal Configuration in The Mesiobuccal Root of The Maxillary First Molar: A Clinical StudyDocumento3 páginasClinical Article Canal Configuration in The Mesiobuccal Root of The Maxillary First Molar: A Clinical Studyperla sofia medina soriaAún no hay calificaciones
- Deboutray 2016Documento8 páginasDeboutray 2016Fitriani MadiAún no hay calificaciones
- !!! Root Canal Morphology and It's Relationship To Endodontic Procedures - Frank J. Vertucci !!!Documento27 páginas!!! Root Canal Morphology and It's Relationship To Endodontic Procedures - Frank J. Vertucci !!!Puscas Madalina100% (1)
- Art Yogesh SirDocumento5 páginasArt Yogesh SirRuchi ShahAún no hay calificaciones
- Art EndoDocumento6 páginasArt EndoVANESSA ALVITRESAún no hay calificaciones
- Imaging in Oral Cancers: Ead and Eck YmposiumDocumento14 páginasImaging in Oral Cancers: Ead and Eck YmposiumHayyu F RachmadhanAún no hay calificaciones
- Branching of Mandibular Canal On Cone BeamDocumento5 páginasBranching of Mandibular Canal On Cone BeamKarina CarlinAún no hay calificaciones
- Jurnal 2Documento8 páginasJurnal 2NissaAún no hay calificaciones
- Evaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyDocumento10 páginasEvaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyPututu PatataAún no hay calificaciones
- Detection of Root Canal Isthmuses in Molars by Map-Reading Dynamic Using CBCT ImagesDocumento6 páginasDetection of Root Canal Isthmuses in Molars by Map-Reading Dynamic Using CBCT ImagesAnny VasquezAún no hay calificaciones
- Canal Mesiovestibular en 1msDocumento5 páginasCanal Mesiovestibular en 1msFiorella AlexandraAún no hay calificaciones
- Mucoceles Dari Rongga Mulut: Serangkaian Kasus Besar (1994-2008) Dan Kajian LiteraturDocumento7 páginasMucoceles Dari Rongga Mulut: Serangkaian Kasus Besar (1994-2008) Dan Kajian LiteraturDhiya Salma AzminidaAún no hay calificaciones
- An Evaluation of Mandibular Canal Variations: A Systematic Review and Meta AnalysisDocumento9 páginasAn Evaluation of Mandibular Canal Variations: A Systematic Review and Meta AnalysisDANTE DELEGUERYAún no hay calificaciones
- Ferreira 2020Documento10 páginasFerreira 2020Dela MedinaAún no hay calificaciones
- The Internal Root Canal Morphology of Single Rooted Mandibular Canines Revealed by Micro ComputedDocumento4 páginasThe Internal Root Canal Morphology of Single Rooted Mandibular Canines Revealed by Micro Computedimran khanAún no hay calificaciones
- OmyxomaDocumento6 páginasOmyxomaClaret TeneAún no hay calificaciones
- A Micro-Computed Tomography Study of The Root Canal Morphology of The Mandibular First Premolar in A Population From Southwestern ChinaDocumento10 páginasA Micro-Computed Tomography Study of The Root Canal Morphology of The Mandibular First Premolar in A Population From Southwestern ChinaNissaAún no hay calificaciones
- Evaluation of Different Treatments For Oroantral Oronasal Communications - Abuabara Et Al PDFDocumento4 páginasEvaluation of Different Treatments For Oroantral Oronasal Communications - Abuabara Et Al PDFVictor HernandezAún no hay calificaciones
- 4.aberrant Root Canal Anatomy in Max 2nd MolarDocumento11 páginas4.aberrant Root Canal Anatomy in Max 2nd MolarSoham DattaAún no hay calificaciones
- Nasal Cavity Shape in Unilateral Choanal Atresia and The Role of Fetal Ventilation in Facial GrowthDocumento6 páginasNasal Cavity Shape in Unilateral Choanal Atresia and The Role of Fetal Ventilation in Facial GrowthNalendra Tri WidhianartoAún no hay calificaciones
- Comparison of Two Protocols For Maxillary Protraction: Bone Anchors Versus Face Mask With Rapid Maxillary ExpansionDocumento8 páginasComparison of Two Protocols For Maxillary Protraction: Bone Anchors Versus Face Mask With Rapid Maxillary ExpansionBeatriz ChilenoAún no hay calificaciones
- Kjod 51 4 250Documento10 páginasKjod 51 4 250utokaAún no hay calificaciones
- 7canals 2Documento7 páginas7canals 2Ruchi ShahAún no hay calificaciones
- The Morphology of Maxillary First and Second Molars Analyzed by Cone-Beam Computed Tomography in A Polish PopulationDocumento7 páginasThe Morphology of Maxillary First and Second Molars Analyzed by Cone-Beam Computed Tomography in A Polish Populationkhaldalfqyh666Aún no hay calificaciones
- !!! Missed Anatomy - Frequency and Clinical Impact !!!Documento32 páginas!!! Missed Anatomy - Frequency and Clinical Impact !!!Puscas MadalinaAún no hay calificaciones
- Prevalence of Radix Entamolaris in Kashmiri PopulationDocumento7 páginasPrevalence of Radix Entamolaris in Kashmiri Populationarshad khandayAún no hay calificaciones
- IndianJRadiolImaging223195-1839113 050631Documento14 páginasIndianJRadiolImaging223195-1839113 050631syedmiskin006Aún no hay calificaciones
- 11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The LiteratureDocumento11 páginas11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The Literaturekochikaghochi100% (1)
- Art OrtoDocumento6 páginasArt OrtoMaripaz Stephania Cabrera ZapataAún no hay calificaciones
- CLasificación de Glosectomias 2019Documento7 páginasCLasificación de Glosectomias 2019Karla Rojas NoeAún no hay calificaciones
- Clasificación GlosectomíasDocumento7 páginasClasificación GlosectomíasAlvaro rivero calleAún no hay calificaciones
- 3 PBDocumento8 páginas3 PBfabian hernandez medinaAún no hay calificaciones
- JjkkkopDocumento3 páginasJjkkkopNurul HidayatiAún no hay calificaciones
- Class III Malocclusion and Bilateral Cross-Bite in An Adult Patient Treated With Miniscrew-Assisted Rapid Palatal Expander and AlignersDocumento16 páginasClass III Malocclusion and Bilateral Cross-Bite in An Adult Patient Treated With Miniscrew-Assisted Rapid Palatal Expander and AlignersMirza GlusacAún no hay calificaciones
- 1-S2.0-S0278239119305518-MainDocumento15 páginas1-S2.0-S0278239119305518-MainALEJANDRA INÉS NIETO ARIASAún no hay calificaciones
- Itsmos en CBCT en Primeras Molares InferioresDocumento9 páginasItsmos en CBCT en Primeras Molares InferioresSaray ValerioAún no hay calificaciones
- Cysts of the Oral and Maxillofacial RegionsDe EverandCysts of the Oral and Maxillofacial RegionsCalificación: 4 de 5 estrellas4/5 (1)
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceDe EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceAún no hay calificaciones
- Benefit-Risk Analysis For Big Data Projects - 2014 PDFDocumento16 páginasBenefit-Risk Analysis For Big Data Projects - 2014 PDFbogdimAún no hay calificaciones
- Present Status and Future Directions Microbiology of Endodontic Infections - 2021Documento19 páginasPresent Status and Future Directions Microbiology of Endodontic Infections - 2021bogdimAún no hay calificaciones
- The Endodontic Complexity Assessment Tool - E-CAT - 2021Documento11 páginasThe Endodontic Complexity Assessment Tool - E-CAT - 2021bogdimAún no hay calificaciones
- Big Data Tutorial Part4Documento41 páginasBig Data Tutorial Part4476Aún no hay calificaciones
- The Development of The Endodontic Complexity Assessment Tool (E-CAT) - 2018Documento193 páginasThe Development of The Endodontic Complexity Assessment Tool (E-CAT) - 2018bogdimAún no hay calificaciones
- Incidence of C-Shaped Root Canal Systems in Mandibular Second Molars in The Native Chinese Population - 2012Documento5 páginasIncidence of C-Shaped Root Canal Systems in Mandibular Second Molars in The Native Chinese Population - 2012bogdimAún no hay calificaciones
- Gardner 04Documento262 páginasGardner 04lunaticseszkaja100% (1)
- Big Data PrivacyDocumento28 páginasBig Data PrivacyMonHskAún no hay calificaciones
- The Britannica Guide To The 100 Most Influential Americans - 2008 PDFDocumento496 páginasThe Britannica Guide To The 100 Most Influential Americans - 2008 PDFbogdimAún no hay calificaciones
- (Dynamic Earth) John P. Rafferty-Storms, Violent Winds, and Earth's Atmosphere-Britannica Educational Publishing (2010) PDFDocumento251 páginas(Dynamic Earth) John P. Rafferty-Storms, Violent Winds, and Earth's Atmosphere-Britannica Educational Publishing (2010) PDFSceptre starAún no hay calificaciones
- Focus On Biodentine - October 2012Documento20 páginasFocus On Biodentine - October 2012bogdimAún no hay calificaciones
- The Last Vikings - 2010 PDFDocumento304 páginasThe Last Vikings - 2010 PDFbogdimAún no hay calificaciones
- The 100 Most Influential Women of All Time The Britannica Guide To The World 039 S Most Influential PeopleDocumento359 páginasThe 100 Most Influential Women of All Time The Britannica Guide To The World 039 S Most Influential PeopleZaw Win100% (3)
- Endocrowns - A Clinical ReportDocumento8 páginasEndocrowns - A Clinical ReportbogdimAún no hay calificaciones
- Interrelationships in The Variability of Root Canal Anatomy Among The Permanent Teeth. A Full-Mouth Approach by Cone-Beam CT - 2016Documento13 páginasInterrelationships in The Variability of Root Canal Anatomy Among The Permanent Teeth. A Full-Mouth Approach by Cone-Beam CT - 2016bogdimAún no hay calificaciones
- .Archivetempcanal and Isthmus Morphology in Mandibular PDFDocumento5 páginas.Archivetempcanal and Isthmus Morphology in Mandibular PDFHilda LiemAún no hay calificaciones
- Micro-CT Analyses of Apical Enlargement and Molar Root Canal ComplexityDocumento9 páginasMicro-CT Analyses of Apical Enlargement and Molar Root Canal ComplexitybogdimAún no hay calificaciones
- Maxillary First Molar With Six CanalsDocumento4 páginasMaxillary First Molar With Six CanalsbogdimAún no hay calificaciones
- Root Canal AnatomyDocumento10 páginasRoot Canal AnatomyNitin MaitinAún no hay calificaciones
- Biomechanical Considerations For The Restoration On Endodontically Treated Teeth. A Systematic Review of The Literature-Part I. Composition and Micro and Macrostructure AlterationsDocumento11 páginasBiomechanical Considerations For The Restoration On Endodontically Treated Teeth. A Systematic Review of The Literature-Part I. Composition and Micro and Macrostructure AlterationsGonzalo Bravo Ahumada100% (1)
- Modern Technologies in Endodontics - 2015Documento8 páginasModern Technologies in Endodontics - 2015bogdimAún no hay calificaciones
- Root Canal MorphologyDocumento5 páginasRoot Canal MorphologyKanika KrishnatreAún no hay calificaciones
- Root MorphologyDocumento9 páginasRoot MorphologycenanolAún no hay calificaciones
- An Optical Investigation of Dentinal Discoloration Due To Commonly Endodontic Sealers, Using The Transmitted Light Polarizing Microscopy and Spectrophotometry - 2016Documento7 páginasAn Optical Investigation of Dentinal Discoloration Due To Commonly Endodontic Sealers, Using The Transmitted Light Polarizing Microscopy and Spectrophotometry - 2016bogdimAún no hay calificaciones
- Biocompatibility Study of Several Esthetic Dental Restorative Materials - 2016Documento5 páginasBiocompatibility Study of Several Esthetic Dental Restorative Materials - 2016bogdimAún no hay calificaciones
- Current Opinions Concerning The Restoration of Endodontically Treated Teeth. Basic Principles PDFDocumento8 páginasCurrent Opinions Concerning The Restoration of Endodontically Treated Teeth. Basic Principles PDFbogdimAún no hay calificaciones
- Comparative Sealing Ability of Three Temporary Coronal Restoration Materials Used For The Access Cavity of Endodontically Treated TeethDocumento2 páginasComparative Sealing Ability of Three Temporary Coronal Restoration Materials Used For The Access Cavity of Endodontically Treated TeethbogdimAún no hay calificaciones
- Current Considerations Concerning Endodontically Treated Teeth: Alteration of Hard Dental Tissues and Biomechanical Properties Following Endodontic TherapyDocumento9 páginasCurrent Considerations Concerning Endodontically Treated Teeth: Alteration of Hard Dental Tissues and Biomechanical Properties Following Endodontic TherapybogdimAún no hay calificaciones
- Doctors MumbaiDocumento6 páginasDoctors Mumbaiutkarsha rane0% (1)
- Unusual Ways Usual DestinationDocumento3 páginasUnusual Ways Usual DestinationLina Saad0% (1)
- Single Visit EndodonticsDocumento6 páginasSingle Visit EndodonticsFathi BanurAún no hay calificaciones
- Cohi Press Release Final DraftDocumento2 páginasCohi Press Release Final Draftapi-599831368Aún no hay calificaciones
- 152-155 Valerio Milana DefDocumento4 páginas152-155 Valerio Milana DefVikas DeepAún no hay calificaciones
- Physicians and Medical SpecialtiesDocumento6 páginasPhysicians and Medical SpecialtiesdianakhyAún no hay calificaciones
- Accidental File SwallowingDocumento6 páginasAccidental File SwallowingShivani DubeyAún no hay calificaciones
- Dentin As A Bonding SubstrateDocumento27 páginasDentin As A Bonding SubstrateAle MonzalvoAún no hay calificaciones
- Textbook of Endodontics, 2nd EditionDocumento555 páginasTextbook of Endodontics, 2nd EditionFizioterapia100% (33)
- A Comparison of One Versus Two Appointment EndodonticDocumento6 páginasA Comparison of One Versus Two Appointment EndodonticShurinam Zaidel Sinain MadariagaAún no hay calificaciones
- DR Nishtha - BDS, MDS, Morth Rcsed Uk - 1Documento6 páginasDR Nishtha - BDS, MDS, Morth Rcsed Uk - 1Nishtha SinghalAún no hay calificaciones
- Restoration of Endodontically Treated TeethDocumento85 páginasRestoration of Endodontically Treated TeethSayak GuptaAún no hay calificaciones
- Endodontic SurgeryDocumento42 páginasEndodontic SurgeryAME DENTAL COLLEGE RAICHUR, KARNATAKAAún no hay calificaciones
- Fee Schedule Yellow (A) UpdatedDocumento2 páginasFee Schedule Yellow (A) Updatedade melly septianaAún no hay calificaciones
- R1a in Vivo Study of Use of Bioceramic MaterialDocumento4 páginasR1a in Vivo Study of Use of Bioceramic MaterialIoana GrigorasAún no hay calificaciones
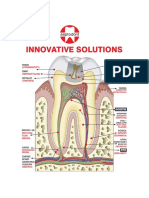
- Innovative Solutions: BiodentineDocumento16 páginasInnovative Solutions: BiodentineRavi KumarAún no hay calificaciones
- Endo-Perio Dilemma A Brief ReviewDocumento10 páginasEndo-Perio Dilemma A Brief ReviewLuisAún no hay calificaciones
- Radix EntomolarisDocumento12 páginasRadix Entomolarisshatakshi rastogiAún no hay calificaciones
- Int Endodontic J - January 1995 - RAY - Periapical Status of Endodontically Treated Teeth in Relation To The TechnicalDocumento8 páginasInt Endodontic J - January 1995 - RAY - Periapical Status of Endodontically Treated Teeth in Relation To The Technicalj sAún no hay calificaciones
- Revascularization-Associated Intracanal Calcification: A Case Report With An 8-Year ReviewDocumento4 páginasRevascularization-Associated Intracanal Calcification: A Case Report With An 8-Year ReviewIvan PolancoAún no hay calificaciones
- Master's in Clinical Dentistry (MClinDent) EndodontologyDocumento8 páginasMaster's in Clinical Dentistry (MClinDent) Endodontologybadar_aqAún no hay calificaciones
- Wytyczne ESE Biologiczne Leczenie MiazgiDocumento12 páginasWytyczne ESE Biologiczne Leczenie MiazgiPaweł SieradzkiAún no hay calificaciones
- Adex Dental Exam Series: Fixed Prosthodontics and EndodonticsDocumento36 páginasAdex Dental Exam Series: Fixed Prosthodontics and EndodonticsmeethaileyyyAún no hay calificaciones
- Principles of Endodontic Surgery: Chapter OutlineDocumento42 páginasPrinciples of Endodontic Surgery: Chapter OutlineFarhan FadhillahAún no hay calificaciones
- Crash Course in EndodonticsDocumento105 páginasCrash Course in Endodonticszakarya hasaninAún no hay calificaciones