También podría gustarte
- Organo Phosphate Poisoning by DR Gireesh Kumar K PDocumento16 páginasOrgano Phosphate Poisoning by DR Gireesh Kumar K PAETCM Emergency medicineAún no hay calificaciones
- Platelet, FFP and Cryoprecipitate Transfusion in Emergency Room by DR Riaz AhamedDocumento31 páginasPlatelet, FFP and Cryoprecipitate Transfusion in Emergency Room by DR Riaz AhamedAETCM Emergency medicineAún no hay calificaciones
- Hepatic Encephalopathy Is by DR Gireesh Kumar K PDocumento16 páginasHepatic Encephalopathy Is by DR Gireesh Kumar K PAETCM Emergency medicineAún no hay calificaciones
- Management of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocumento13 páginasManagement of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaSreekrishnan TrikkurAún no hay calificaciones
- Neutropenia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocumento10 páginasNeutropenia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaSreekrishnan TrikkurAún no hay calificaciones
- Haemolytic Anemia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocumento14 páginasHaemolytic Anemia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaAETCM Emergency medicineAún no hay calificaciones
- Innovation EDDocumento32 páginasInnovation EDAETCM Emergency medicineAún no hay calificaciones
- Acute Myocardial Infarction by DR Gireesh Kumar K PDocumento18 páginasAcute Myocardial Infarction by DR Gireesh Kumar K PAETCM Emergency medicine50% (2)
- DR Aida Lombok 3 Mei 2017 - HisfarsiDocumento39 páginasDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamAún no hay calificaciones
- KegawatdaruratanDocumento164 páginasKegawatdaruratanmeida astriani gozaziAún no hay calificaciones
- Neutropenia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocumento10 páginasNeutropenia by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaSreekrishnan TrikkurAún no hay calificaciones
- Ngaji Arrythmia Cordis 3Documento122 páginasNgaji Arrythmia Cordis 3Dhita Dwi NandaAún no hay calificaciones
- Delirium in critically ill patients: Should we worryDocumento37 páginasDelirium in critically ill patients: Should we worrySanj.etcAún no hay calificaciones
- Hypertensive Emergencies: BY: Dr. Imtiyaz Hashim (PGR) Dr. Khalida Baloch (Ho)Documento31 páginasHypertensive Emergencies: BY: Dr. Imtiyaz Hashim (PGR) Dr. Khalida Baloch (Ho)امتیاز ہاشم بزنجوAún no hay calificaciones
- Clinical Order Set DKA AdultDocumento2 páginasClinical Order Set DKA AdultBashar Al-HamaidehAún no hay calificaciones
- Heart Failure Topic DiscussionDocumento11 páginasHeart Failure Topic Discussionapi-665372449Aún no hay calificaciones
- Evaluation and Management of Suspected Sepsis and Septic by DR Gireesh Kumar K PDocumento36 páginasEvaluation and Management of Suspected Sepsis and Septic by DR Gireesh Kumar K PSreekrishnan TrikkurAún no hay calificaciones
- Hemophilia: Factor IX (Hemophilia B)Documento38 páginasHemophilia: Factor IX (Hemophilia B)Jhvhjgj JhhgtyAún no hay calificaciones
- PATHOPHYSIOLOGY OF SHOCKDocumento56 páginasPATHOPHYSIOLOGY OF SHOCKDr. Haricharan AAún no hay calificaciones
- ECG Changes in Drug and Electrolyte AbnormalitiesDocumento28 páginasECG Changes in Drug and Electrolyte AbnormalitiesNachiket Vijay PotdarAún no hay calificaciones
- Critical Care Drugs OverviewDocumento23 páginasCritical Care Drugs OverviewAsri Ernadi100% (1)
- CHPT 70 Respiratory Part 2Documento56 páginasCHPT 70 Respiratory Part 2helen brockAún no hay calificaciones
- Acute Renal FailureDocumento5 páginasAcute Renal FailureSalman KhanAún no hay calificaciones
- Stroke ManagementDocumento18 páginasStroke ManagementAETCM Emergency medicineAún no hay calificaciones
- Hypovolemic ShockDocumento21 páginasHypovolemic ShockOlga GoryachevaAún no hay calificaciones
- Invasive Pulmonary Aspergi Llosis: Seminars in Respiratory and Critical Care MedicineDocumento24 páginasInvasive Pulmonary Aspergi Llosis: Seminars in Respiratory and Critical Care MedicineChengShiun ShiueAún no hay calificaciones
- Drugs Used for Treatment Stable Angina PectorisDocumento29 páginasDrugs Used for Treatment Stable Angina PectorisAditya Andra PerdanaAún no hay calificaciones
- Hyperglycemia Crisis: Dr. Netty NurnaningtyasDocumento34 páginasHyperglycemia Crisis: Dr. Netty Nurnaningtyasnetty nurnaningtyasAún no hay calificaciones
- Pyrexia of Unknown OriginDocumento81 páginasPyrexia of Unknown OriginJithin Bhagavati Kalam100% (1)
- PheochromocytomaDocumento74 páginasPheochromocytomamichaelAún no hay calificaciones
- Managing HypokalemiaDocumento26 páginasManaging HypokalemiaClarisse Cloie LamberteAún no hay calificaciones
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDocumento34 páginasHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiAún no hay calificaciones
- Right Heart Catheterization, NicvdDocumento17 páginasRight Heart Catheterization, NicvdNavojit ChowdhuryAún no hay calificaciones
- Potassium ParticipantsDocumento21 páginasPotassium ParticipantsSkylar IvyAún no hay calificaciones
- Pericardial Diseases 3rd Yr BMTDocumento38 páginasPericardial Diseases 3rd Yr BMT211941103014100% (1)
- Coronary Artery Disease Cad2Documento182 páginasCoronary Artery Disease Cad2Mamot MotAún no hay calificaciones
- Ch-13 Drugs Used in Heart FailureDocumento49 páginasCh-13 Drugs Used in Heart FailureShabrin SadikhAún no hay calificaciones
- ARRHYTHMIADocumento82 páginasARRHYTHMIAjiluAún no hay calificaciones
- Oleander PoisoningDocumento19 páginasOleander PoisoningAnbu Arasan100% (1)
- Ecg Pathology 02Documento95 páginasEcg Pathology 02Andi MP Manurung100% (1)
- Quality of CPRDocumento47 páginasQuality of CPRSreekrishnan TrikkurAún no hay calificaciones
- Diabetic Nephropathy: Assisstant Professor Dr. Mihaela-Dora DonciuDocumento65 páginasDiabetic Nephropathy: Assisstant Professor Dr. Mihaela-Dora DonciuFloreaAndreiAún no hay calificaciones
- Approach To HyponatremiaDocumento47 páginasApproach To HyponatremiaRajiv MedankiAún no hay calificaciones
- Cardiomyopathy: Leonard Shaju Joisy AloorDocumento34 páginasCardiomyopathy: Leonard Shaju Joisy AloorJoisy AloorAún no hay calificaciones
- Hyponatremia in Children 03.19.2010Documento23 páginasHyponatremia in Children 03.19.2010Emily EresumaAún no hay calificaciones
- Management of Hypertensive Emergency and UrgencyDocumento20 páginasManagement of Hypertensive Emergency and UrgencyOersted EdwardAún no hay calificaciones
- AlcoholDocumento20 páginasAlcoholrecklesspeshal2058100% (1)
- SepsisDocumento33 páginasSepsisv_vijayakanth7656Aún no hay calificaciones
- An Overview Of: Acute Kidney Injury (Aki: Hasan BasriDocumento22 páginasAn Overview Of: Acute Kidney Injury (Aki: Hasan BasriDz PutraAún no hay calificaciones
- AnginaDocumento12 páginasAnginaDr-Sanjay SinghaniaAún no hay calificaciones
- Hypertensive EmergenciesDocumento49 páginasHypertensive EmergenciesSafa Abdualrahaman Ali HamadAún no hay calificaciones
- Acute Treatment of Hypocalcaemia (Adults)Documento2 páginasAcute Treatment of Hypocalcaemia (Adults)Ahed WarwarAún no hay calificaciones
- NOAC ChartDocumento2 páginasNOAC Chartsgod34Aún no hay calificaciones
- Hypertension LecturesDocumento65 páginasHypertension LecturesAdebisiAún no hay calificaciones
- STEP HPEF Trial NEJm 2023Documento16 páginasSTEP HPEF Trial NEJm 2023felipeAún no hay calificaciones
- Evaluation of Liver FunctionDocumento64 páginasEvaluation of Liver FunctionMustafa KhandgawiAún no hay calificaciones
- Emergency ECG changes in hyperkalemiaDocumento7 páginasEmergency ECG changes in hyperkalemiaAlok yadav100% (1)
- Heart FailureDocumento44 páginasHeart FailureSalman Habeeb100% (6)
- Cardiac Heart Failure Guide: Causes, Symptoms & Nursing CareDocumento43 páginasCardiac Heart Failure Guide: Causes, Symptoms & Nursing CareCindy DeliaAún no hay calificaciones
- Session 24 Heart FailureDocumento15 páginasSession 24 Heart Failuredreampurpose97Aún no hay calificaciones
- SARS-CoV2 Ag Kit - Biosensor PDFDocumento2 páginasSARS-CoV2 Ag Kit - Biosensor PDFAETCM Emergency medicineAún no hay calificaciones
- Post Exposure Prophylaxis in HIVDocumento9 páginasPost Exposure Prophylaxis in HIVAETCM Emergency medicineAún no hay calificaciones
- SVT PediatricDocumento1 páginaSVT PediatricAETCM Emergency medicineAún no hay calificaciones
- SARS-CoV2 Ag Kit - Biosensor PDFDocumento2 páginasSARS-CoV2 Ag Kit - Biosensor PDFAETCM Emergency medicineAún no hay calificaciones
- Acute Myocardial Infarction by DR Gireesh Kumar K PDocumento18 páginasAcute Myocardial Infarction by DR Gireesh Kumar K PAETCM Emergency medicine50% (2)
- Stroke ManagementDocumento18 páginasStroke ManagementAETCM Emergency medicineAún no hay calificaciones
- Pulmonary EmbolosmDocumento15 páginasPulmonary EmbolosmAETCM Emergency medicineAún no hay calificaciones
- SARS-CoV2 Ag Kit - Biosensor PDFDocumento2 páginasSARS-CoV2 Ag Kit - Biosensor PDFAETCM Emergency medicineAún no hay calificaciones
- Snake Bite ToxiconDocumento14 páginasSnake Bite ToxiconAETCM Emergency medicine100% (1)
- Stroke ManagementDocumento18 páginasStroke ManagementAETCM Emergency medicineAún no hay calificaciones
- HyponatremiaDocumento19 páginasHyponatremiaAETCM Emergency medicine100% (1)
- Acute Exacerbation of COPD by DR Gireesh Kumar KPDocumento12 páginasAcute Exacerbation of COPD by DR Gireesh Kumar KPAETCM Emergency medicineAún no hay calificaciones
- Pulmonary EmbolosmDocumento15 páginasPulmonary EmbolosmAETCM Emergency medicineAún no hay calificaciones
- HyponatremiaDocumento19 páginasHyponatremiaAETCM Emergency medicine100% (1)
- Bells Palsy by DR Gireesh Kumar K PDocumento6 páginasBells Palsy by DR Gireesh Kumar K PAETCM Emergency medicineAún no hay calificaciones
- Post Exposure Prophylaxis in HIV by DR Gireesh Kumar KPDocumento9 páginasPost Exposure Prophylaxis in HIV by DR Gireesh Kumar KPAETCM Emergency medicineAún no hay calificaciones
- Status Epileptic Us by DR Gireesh Kumar K PDocumento18 páginasStatus Epileptic Us by DR Gireesh Kumar K PAETCM Emergency medicineAún no hay calificaciones
- Acute Asthma by DR Gireesh Kumar KPDocumento15 páginasAcute Asthma by DR Gireesh Kumar KPAETCM Emergency medicineAún no hay calificaciones
- Status Epilepticus by DR Gireesh Kumar K PDocumento18 páginasStatus Epilepticus by DR Gireesh Kumar K PAETCM Emergency medicineAún no hay calificaciones
- Innovation EDDocumento32 páginasInnovation EDAETCM Emergency medicineAún no hay calificaciones
- Guillain Barre Syndrome by DR Gireesh Kumar K PDocumento10 páginasGuillain Barre Syndrome by DR Gireesh Kumar K PAETCM Emergency medicineAún no hay calificaciones
- Pulmonary Edema by DR Gireesh Kumar K PDocumento16 páginasPulmonary Edema by DR Gireesh Kumar K PAETCM Emergency medicineAún no hay calificaciones
- Nipah Viral Infection by DR Gireesh Kumar KPDocumento10 páginasNipah Viral Infection by DR Gireesh Kumar KPAETCM Emergency medicineAún no hay calificaciones
- Snake Bite by DR Gireesh Kumar KPDocumento13 páginasSnake Bite by DR Gireesh Kumar KPAETCM Emergency medicineAún no hay calificaciones
- Hyperkalemia by DR Gireesh Kumar K PDocumento15 páginasHyperkalemia by DR Gireesh Kumar K PAETCM Emergency medicineAún no hay calificaciones
- Diabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiDocumento23 páginasDiabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiSreekrishnan Trikkur100% (2)
- Distinguishing TRALI and TACODocumento6 páginasDistinguishing TRALI and TACOl1o2stAún no hay calificaciones
- Gnaps EmedicineDocumento13 páginasGnaps Emedicineharyanti lupitaAún no hay calificaciones
- Emergency Treatment of Acute Heart FailureDocumento9 páginasEmergency Treatment of Acute Heart FailureAlanAún no hay calificaciones
- Chan, Johnson - TreatmentGuidelines PDFDocumento0 páginasChan, Johnson - TreatmentGuidelines PDFBogdan CarabasAún no hay calificaciones
- Evaluation of Dyspneic PatientDocumento15 páginasEvaluation of Dyspneic Patientcamila perillaAún no hay calificaciones
- Normal Lab Values Guide in 40 CharactersDocumento37 páginasNormal Lab Values Guide in 40 CharactersKelly Camero ÜAún no hay calificaciones
- Soal MAYO Yg KeluarDocumento8 páginasSoal MAYO Yg KeluardoktersaktiAún no hay calificaciones
- Nt-Probnp: The Gold Standard Biomarker in Heart FailureDocumento3 páginasNt-Probnp: The Gold Standard Biomarker in Heart FailureRiuin23Aún no hay calificaciones
- Renal Siadh Di CSWDocumento54 páginasRenal Siadh Di CSWRizka Nurul Firdaus100% (1)
- NeseritideDocumento28 páginasNeseritideNavojit Chowdhury100% (1)
- Cardiac Enzymes - KulDocumento39 páginasCardiac Enzymes - KulAnonymous J1iWk2xAún no hay calificaciones
- Methanol, Anhydrous, 99.8% - CH3OH - Sigma-AldrichDocumento5 páginasMethanol, Anhydrous, 99.8% - CH3OH - Sigma-AldrichmodusAún no hay calificaciones
- MAT 2379 (A), Introduction To Biostatistics.: Assignment 1 (5 Questions)Documento6 páginasMAT 2379 (A), Introduction To Biostatistics.: Assignment 1 (5 Questions)tabarekAún no hay calificaciones
- Risk For Decreased Cardiac OutputDocumento4 páginasRisk For Decreased Cardiac Outputapi-283482759Aún no hay calificaciones
- Acute Decompensated Heart FailureDocumento36 páginasAcute Decompensated Heart FailureKartika PelangoAún no hay calificaciones
- Brain Natriuretic PeptideDocumento8 páginasBrain Natriuretic PeptidegunawanAún no hay calificaciones
- Physiologic Changes During Pregnancy and DeliveryDocumento13 páginasPhysiologic Changes During Pregnancy and DeliveryBudi Khang100% (1)
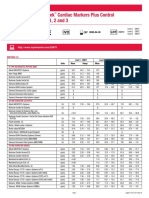
- Liquichek Cardiac Markers Plus Control Levels 1, 2 and 3: MethodDocumento4 páginasLiquichek Cardiac Markers Plus Control Levels 1, 2 and 3: MethodSaifoel RahmanAún no hay calificaciones
- Encyclopedia of Biological Chemistry - Vol - 3Documento848 páginasEncyclopedia of Biological Chemistry - Vol - 3joshigauta100% (1)
- Heart Failure PathophysiologyDocumento11 páginasHeart Failure PathophysiologyNur HaidagAún no hay calificaciones
- Cardio SNAP-BNP NT-proBNP IdexxDocumento4 páginasCardio SNAP-BNP NT-proBNP IdexxXenia FernandezAún no hay calificaciones
- Attending COPD Exacerbation ModuleDocumento9 páginasAttending COPD Exacerbation ModuleJonathan AiresAún no hay calificaciones
- CCFDocumento60 páginasCCFVajja SwatiAún no hay calificaciones
- Masterclass Book Part 2Documento367 páginasMasterclass Book Part 2Eng Kian Ng100% (5)
- Cerebral Salt Wasting Syndrome ReviewDocumento6 páginasCerebral Salt Wasting Syndrome ReviewSoewira Sastra100% (1)
- International Journal of Cardiology: ArticleinfoDocumento5 páginasInternational Journal of Cardiology: ArticleinfoWiyosa RusdiAún no hay calificaciones
- Guidelines For The Diagnosis and Treatment of Chronic Heart FailureDocumento26 páginasGuidelines For The Diagnosis and Treatment of Chronic Heart FailurecubewormAún no hay calificaciones
- Assessment of Breathlessness Clinical Pathway Assessment HandoutDocumento8 páginasAssessment of Breathlessness Clinical Pathway Assessment HandoutShivaniAún no hay calificaciones
- Heart Failure. BraunwaldDocumento20 páginasHeart Failure. Braunwaldjujuju26Aún no hay calificaciones
- Modern Management of Cardiogenic Pulmonary Edema: Amal Mattu, MD, Joseph P. Martinez, MD, Brian S. Kelly, MDDocumento21 páginasModern Management of Cardiogenic Pulmonary Edema: Amal Mattu, MD, Joseph P. Martinez, MD, Brian S. Kelly, MDJoni MokodoAún no hay calificaciones