También podría gustarte
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Exercise 23 - Sulfur OintmentDocumento4 páginasExercise 23 - Sulfur OintmentmaimaiAún no hay calificaciones
- Gravity Based Foundations For Offshore Wind FarmsDocumento121 páginasGravity Based Foundations For Offshore Wind FarmsBent1988Aún no hay calificaciones
- Journal of Psychosomatic ResearchDocumento7 páginasJournal of Psychosomatic Researchnermal93Aún no hay calificaciones
- 2011 Koc - MPV InflameDocumento4 páginas2011 Koc - MPV Inflamenermal93Aún no hay calificaciones
- Journal of Psychosomatic Research: Asish Subedi, Krishna Pokharel, Birendra Prasad Sah, Pashupati ChaudharyDocumento6 páginasJournal of Psychosomatic Research: Asish Subedi, Krishna Pokharel, Birendra Prasad Sah, Pashupati Chaudharynermal93Aún no hay calificaciones
- 2020 Nemeroff - DeP ReviewDocumento15 páginas2020 Nemeroff - DeP Reviewnermal93Aún no hay calificaciones
- 2020 Waszkiwicz - Biomarker Psychiatrci DisorderDocumento6 páginas2020 Waszkiwicz - Biomarker Psychiatrci Disordernermal93Aún no hay calificaciones
- 2016 Agli Frecnh PDFDocumento13 páginas2016 Agli Frecnh PDFnermal93Aún no hay calificaciones
- 2012 Luchettii - Validation of The Duke Religion Index DUREL PORTUGESEDocumento9 páginas2012 Luchettii - Validation of The Duke Religion Index DUREL PORTUGESEnermal93Aún no hay calificaciones
- Walker2007 PDFDocumento11 páginasWalker2007 PDFnermal93Aún no hay calificaciones
- Effects of Modeling Rote Versus Varied Responses On Response Variability and Skill Acquisition During Discrete-Trial InstructionDocumento16 páginasEffects of Modeling Rote Versus Varied Responses On Response Variability and Skill Acquisition During Discrete-Trial Instructionnermal93Aún no hay calificaciones
- 2015 Coban PDFDocumento11 páginas2015 Coban PDFnermal93Aún no hay calificaciones
- Journal of A Ffective Disorders: Ling-Yi Wang, Jen-Huai Chiang, Shih-Fen Chen, Yu-Chih ShenDocumento7 páginasJournal of A Ffective Disorders: Ling-Yi Wang, Jen-Huai Chiang, Shih-Fen Chen, Yu-Chih Shennermal93Aún no hay calificaciones
- Progress in Neuro-Psychopharmacology & Biological PsychiatryDocumento10 páginasProgress in Neuro-Psychopharmacology & Biological Psychiatrynermal93Aún no hay calificaciones
- 2017 PéterfiDocumento9 páginas2017 Péterfinermal93Aún no hay calificaciones
- Clinical: Exposure To Solvents in Female Patients With SclerodermaDocumento5 páginasClinical: Exposure To Solvents in Female Patients With Sclerodermanermal93Aún no hay calificaciones
- Journal of Ginseng Research: Seungyeop Lee, Dong-Kwon RheeDocumento6 páginasJournal of Ginseng Research: Seungyeop Lee, Dong-Kwon Rheenermal93Aún no hay calificaciones
- 1 s2.0 S088915910700027X Main PDFDocumento10 páginas1 s2.0 S088915910700027X Main PDFnermal93Aún no hay calificaciones
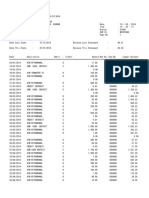
- Bank Statement SampleDocumento6 páginasBank Statement SampleRovern Keith Oro CuencaAún no hay calificaciones
- August 2015Documento96 páginasAugust 2015Cleaner MagazineAún no hay calificaciones
- Pega AcademyDocumento10 páginasPega AcademySasidharAún no hay calificaciones
- Aluminium Extrusion Industry in IndiaDocumento3 páginasAluminium Extrusion Industry in Indiakalan45Aún no hay calificaciones
- Codex Standard EnglishDocumento4 páginasCodex Standard EnglishTriyaniAún no hay calificaciones
- Liga NG Mga Barangay: Resolution No. 30Documento2 páginasLiga NG Mga Barangay: Resolution No. 30Rey PerezAún no hay calificaciones
- Automatic Stair Climbing Wheelchair: Professional Trends in Industrial and Systems Engineering (PTISE)Documento7 páginasAutomatic Stair Climbing Wheelchair: Professional Trends in Industrial and Systems Engineering (PTISE)Abdelrahman MahmoudAún no hay calificaciones
- BreezeAIR 8000 Data SheetDocumento2 páginasBreezeAIR 8000 Data Sheetalfasukarno100% (1)
- Dmta 20043 01en Omniscan SX UserDocumento90 páginasDmta 20043 01en Omniscan SX UserwenhuaAún no hay calificaciones
- STM Series Solar ControllerDocumento2 páginasSTM Series Solar ControllerFaris KedirAún no hay calificaciones
- Certification and LettersDocumento6 páginasCertification and LettersReimar FerrarenAún no hay calificaciones
- Customer Satisfaction-ICICI Bank-Priyanka DhamijaDocumento85 páginasCustomer Satisfaction-ICICI Bank-Priyanka DhamijaVarun GuptaAún no hay calificaciones
- Supreme Court of The United StatesDocumento296 páginasSupreme Court of The United StatesABC News PoliticsAún no hay calificaciones
- Question Bank For Vlsi LabDocumento4 páginasQuestion Bank For Vlsi LabSav ThaAún no hay calificaciones
- Sworn Statement of Assets, Liabilities and Net WorthDocumento3 páginasSworn Statement of Assets, Liabilities and Net WorthShelby AntonioAún no hay calificaciones
- Health, Safety & Environment: Refer NumberDocumento2 páginasHealth, Safety & Environment: Refer NumbergilAún no hay calificaciones
- A Winning Formula: Debrief For The Asda Case (Chapter 14, Shaping Implementation Strategies) The Asda CaseDocumento6 páginasA Winning Formula: Debrief For The Asda Case (Chapter 14, Shaping Implementation Strategies) The Asda CaseSpend ThriftAún no hay calificaciones
- BSBOPS601 Develop Implement Business Plans - SDocumento91 páginasBSBOPS601 Develop Implement Business Plans - SSudha BarahiAún no hay calificaciones
- Residential BuildingDocumento5 páginasResidential Buildingkamaldeep singhAún no hay calificaciones
- Health Informatics SDocumento4 páginasHealth Informatics SnourhanAún no hay calificaciones
- Bismillah SpeechDocumento2 páginasBismillah SpeechanggiAún no hay calificaciones
- Gmo EssayDocumento4 páginasGmo Essayapi-270707439Aún no hay calificaciones
- WHO Partograph Study Lancet 1994Documento6 páginasWHO Partograph Study Lancet 1994Dewi PradnyaAún no hay calificaciones
- Dreamweaver Lure v. Heyne - ComplaintDocumento27 páginasDreamweaver Lure v. Heyne - ComplaintSarah BursteinAún no hay calificaciones
- Interest Rates and Bond Valuation: All Rights ReservedDocumento22 páginasInterest Rates and Bond Valuation: All Rights ReservedAnonymous f7wV1lQKRAún no hay calificaciones
- B.ST Case Study Class 12Documento214 páginasB.ST Case Study Class 12Anishka Rathor100% (1)
- Design of Flyback Transformers and Filter Inductor by Lioyd H.dixon, Jr. Slup076Documento11 páginasDesign of Flyback Transformers and Filter Inductor by Lioyd H.dixon, Jr. Slup076Burlacu AndreiAún no hay calificaciones
- Fr-E700 Instruction Manual (Basic)Documento155 páginasFr-E700 Instruction Manual (Basic)DeTiEnamoradoAún no hay calificaciones