También podría gustarte
- Depigmentasi Gingiva Menggunakan Laser Erbium Doped Yitrium-Alumunium-garnetDocumento5 páginasDepigmentasi Gingiva Menggunakan Laser Erbium Doped Yitrium-Alumunium-garnetleilyanisariAún no hay calificaciones
- DFDGDocumento1 páginaDFDGleilyanisariAún no hay calificaciones
- 07-Adlin Nadia (Siap) PDFDocumento4 páginas07-Adlin Nadia (Siap) PDFleilyanisariAún no hay calificaciones
- BBVBMHVBVGCGCBVN N BCGHCGCHVKHVKVKHDocumento1 páginaBBVBMHVBVGCGCBVN N BCGHCGCHVKHVKVKHleilyanisariAún no hay calificaciones
- Jced 4 E167Documento3 páginasJced 4 E167leilyanisariAún no hay calificaciones
- Masking Conventional Metallic Cast Post For Enhancing EstheticsDocumento5 páginasMasking Conventional Metallic Cast Post For Enhancing EstheticsleilyanisariAún no hay calificaciones
- Treatment of Postherpetic Neuralgia With Low Level Laser TherapyDocumento6 páginasTreatment of Postherpetic Neuralgia With Low Level Laser TherapyleilyanisariAún no hay calificaciones
- 273 540 1 SMDocumento7 páginas273 540 1 SMJihan BusniaAún no hay calificaciones
- Compendium August 1997 Esthetic Crown Lentheing For Maxillary Anterior Teeth1Documento7 páginasCompendium August 1997 Esthetic Crown Lentheing For Maxillary Anterior Teeth1leilyanisariAún no hay calificaciones
- Compendium August 1997 Esthetic Crown Lentheing For Maxillary Anterior Teeth1Documento7 páginasCompendium August 1997 Esthetic Crown Lentheing For Maxillary Anterior Teeth1leilyanisariAún no hay calificaciones
- Masking Conventional Metallic Cast Post For Enhancing EstheticsDocumento5 páginasMasking Conventional Metallic Cast Post For Enhancing EstheticsleilyanisariAún no hay calificaciones
- Removing Bridge PDFDocumento6 páginasRemoving Bridge PDFElbanus WatriAún no hay calificaciones
- Removing Bridge PDFDocumento6 páginasRemoving Bridge PDFElbanus WatriAún no hay calificaciones
- Masking Conventional Metallic Cast Post For Enhancing EstheticsDocumento5 páginasMasking Conventional Metallic Cast Post For Enhancing EstheticsleilyanisariAún no hay calificaciones
- 152.255 Crown N Bridges LowDocumento76 páginas152.255 Crown N Bridges LowleilyanisariAún no hay calificaciones
- Compendium August 1997 Esthetic Crown Lentheing For Maxillary Anterior Teeth1Documento7 páginasCompendium August 1997 Esthetic Crown Lentheing For Maxillary Anterior Teeth1leilyanisariAún no hay calificaciones
- Compendium August 1997 Esthetic Crown Lentheing For Maxillary Anterior Teeth1 PDFDocumento11 páginasCompendium August 1997 Esthetic Crown Lentheing For Maxillary Anterior Teeth1 PDFleilyanisariAún no hay calificaciones
- Dental Surgery in Anticoagulated PatientsDocumento9 páginasDental Surgery in Anticoagulated PatientsleilyanisariAún no hay calificaciones
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5782)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- SG2 08 AsbestosDocumento6 páginasSG2 08 AsbestosDaniel SarmientoAún no hay calificaciones
- Dorothy Johnson PosterDocumento1 páginaDorothy Johnson Posterapi-519455077Aún no hay calificaciones
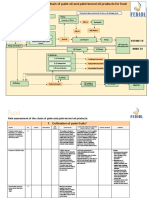
- Risk Assessment Palm Food FEDIOL Final 160522Documento18 páginasRisk Assessment Palm Food FEDIOL Final 160522Jayashri chitteAún no hay calificaciones
- Lahore Debating Gala 2022 MUN ConferenceDocumento8 páginasLahore Debating Gala 2022 MUN ConferenceWahid ShafiqAún no hay calificaciones
- Zambia Daily Mail, Monday, January 3, 2022Documento16 páginasZambia Daily Mail, Monday, January 3, 2022Mulenga MwaleAún no hay calificaciones
- Health PlanningDocumento46 páginasHealth PlanningJems Negn KeziewAún no hay calificaciones
- ESADocumento31 páginasESAssourabAún no hay calificaciones
- Ace Hot Work Permit Application Form PDFDocumento3 páginasAce Hot Work Permit Application Form PDFkevin100% (1)
- File Jurnal Infeksi NosokomialDocumento12 páginasFile Jurnal Infeksi Nosokomialirmayani channelAún no hay calificaciones
- Hypertension GuidelinesDocumento33 páginasHypertension GuidelinesErlinda NRAAún no hay calificaciones
- Foai Fda PDFDocumento3 páginasFoai Fda PDFMadhuriAún no hay calificaciones
- SF 8 Learner's Basic Health and Nutrition ReportDocumento2 páginasSF 8 Learner's Basic Health and Nutrition ReportMichael LegaspiAún no hay calificaciones
- Local Exhaust Ventilation (LEV) (PDF 110KB) PDFDocumento8 páginasLocal Exhaust Ventilation (LEV) (PDF 110KB) PDFvanyoAún no hay calificaciones
- Discover True NorthDocumento7 páginasDiscover True NorthesemAún no hay calificaciones
- Autophagy, Anoikis, Ferroptosis, Necroptosis, and Endoplasmic Reticulum Stress - Potential Applications in Melanoma TherapyDocumento9 páginasAutophagy, Anoikis, Ferroptosis, Necroptosis, and Endoplasmic Reticulum Stress - Potential Applications in Melanoma TherapyEstrella BenitoAún no hay calificaciones
- Maklumat Vaksinasi: Vaccination DetailsDocumento2 páginasMaklumat Vaksinasi: Vaccination Detailshendry anandanAún no hay calificaciones
- Corbett Circle Theorems Textbook ExerciseDocumento11 páginasCorbett Circle Theorems Textbook Exercisekdebipershad100% (1)
- Physio Personal Statement 2Documento1 páginaPhysio Personal Statement 2YB chiu100% (1)
- Healthcare Goes Mobile Evolution of Teleconsultation and e Pharmacy in New NormalDocumento66 páginasHealthcare Goes Mobile Evolution of Teleconsultation and e Pharmacy in New NormalRahul AgarwalAún no hay calificaciones
- Science and Health Com CollegeDocumento14 páginasScience and Health Com CollegeJeyyAún no hay calificaciones
- Feasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentDocumento9 páginasFeasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentAhmed RamzyAún no hay calificaciones
- Doxofylline Drug StudyDocumento2 páginasDoxofylline Drug StudyArabelle GO67% (3)
- Module Four Wellness PlanDocumento13 páginasModule Four Wellness Planso drippy customsAún no hay calificaciones
- ANATOM 64 Precision FinalDocumento12 páginasANATOM 64 Precision Finaljcdavidm2000Aún no hay calificaciones
- A.Haleem (2020) Areas of Academic Research With The Impact of COVID-19Documento8 páginasA.Haleem (2020) Areas of Academic Research With The Impact of COVID-19Azizan RamlyAún no hay calificaciones
- October JournalDocumento36 páginasOctober Journalrammvr05Aún no hay calificaciones
- Maimonides Medical Center - 2021-2022Documento1 páginaMaimonides Medical Center - 2021-2022sal palAún no hay calificaciones
- IELTS Writing Task 2 Actual Test Sep To Dec 2021-Đã M KhóaDocumento256 páginasIELTS Writing Task 2 Actual Test Sep To Dec 2021-Đã M KhóaNguyen HoangAún no hay calificaciones
- Ranunculus K DeficiencyDocumento4 páginasRanunculus K DeficiencysilviafoteaAún no hay calificaciones
- Colonialism and Development Final Version-1Documento29 páginasColonialism and Development Final Version-1salma AkhtarAún no hay calificaciones