También podría gustarte
- Male Physique Template Shoulder and Arm 5 DaysDocumento3 páginasMale Physique Template Shoulder and Arm 5 DaysFrancisco Coutinho40% (5)
- Anatomical Study of Jiu Jitsu Joint LocksDocumento111 páginasAnatomical Study of Jiu Jitsu Joint LocksOuvertureFacile100% (6)
- 18 Carpal Bone FracturesDocumento69 páginas18 Carpal Bone FracturesAdina BotezAún no hay calificaciones
- Examen Ortopedico InfantilDocumento21 páginasExamen Ortopedico InfantilSebastian CamiloAún no hay calificaciones
- InTech-Management of Bone Loss in Primary and Revision Knee Replacement SurgeryDocumento25 páginasInTech-Management of Bone Loss in Primary and Revision Knee Replacement SurgerySagaram ShashidarAún no hay calificaciones
- Coste Et Al. - 1968 - Rheumatoid ForefootDocumento2 páginasCoste Et Al. - 1968 - Rheumatoid ForefootYuki SATAKEAún no hay calificaciones
- Remodeling of Femoral StemDocumento24 páginasRemodeling of Femoral StemdabeeraliAún no hay calificaciones
- Illustration of Implants in Total Knee ReplacementDocumento5 páginasIllustration of Implants in Total Knee ReplacementInternational Journal of Innovative Science and Research TechnologyAún no hay calificaciones
- Ehlinger (2010)Documento6 páginasEhlinger (2010)TommysAún no hay calificaciones
- Ankle Fractures in Adults - UpToDateDocumento50 páginasAnkle Fractures in Adults - UpToDateJose LuceroAún no hay calificaciones
- Fixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFDocumento4 páginasFixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFThomas BowersAún no hay calificaciones
- 10.1177 1941738110397875 PDFDocumento16 páginas10.1177 1941738110397875 PDFalwy sugiartoAún no hay calificaciones
- Metatarsophangeal Joint Instability of The Lesser ToesDocumento7 páginasMetatarsophangeal Joint Instability of The Lesser ToestabareeAún no hay calificaciones
- Tka ValgusDocumento11 páginasTka ValgusOvidiu RusuAún no hay calificaciones
- Orthopedic Hardware and ComplicationsDocumento15 páginasOrthopedic Hardware and ComplicationsItstineeAún no hay calificaciones
- Tibial Plateau Fracture: Anatomy, Diagnosis and Management: Doctors in TrainingDocumento9 páginasTibial Plateau Fracture: Anatomy, Diagnosis and Management: Doctors in TrainingChấm TrấmAún no hay calificaciones
- Comminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewDocumento7 páginasComminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewGustavoBecerraAún no hay calificaciones
- Rehabilitation of Knee Injuries: Robert C. Manske and Mark V. PaternoDocumento23 páginasRehabilitation of Knee Injuries: Robert C. Manske and Mark V. PaternoYMatosAún no hay calificaciones
- Deformidades Antepie ReumatoideoDocumento11 páginasDeformidades Antepie ReumatoideoMercedesBenítezSeculAún no hay calificaciones
- Proximal Tibial Fractures in AdultsDocumento4 páginasProximal Tibial Fractures in AdultsAbdusSomadAún no hay calificaciones
- Indicaciones de La Técnica de Weil PDFDocumento4 páginasIndicaciones de La Técnica de Weil PDFlinc9Aún no hay calificaciones
- Schreibman AnkleTrauma ARRS 08Documento10 páginasSchreibman AnkleTrauma ARRS 08AndykaYayanSetiawanAún no hay calificaciones
- MatthewVaracalloMD TotalKneeReplacementTKRTechniques StatPearls NCBIBookshelfDocumento14 páginasMatthewVaracalloMD TotalKneeReplacementTKRTechniques StatPearls NCBIBookshelfDiego Alvaro Esquivel RomeroAún no hay calificaciones
- Foot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Documento15 páginasFoot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Biblioteca Centro Médico De Mar del PlataAún no hay calificaciones
- 1 s2.0 S2212628723000269 MainDocumento7 páginas1 s2.0 S2212628723000269 MainYordhanno Xavier Fallaque RuizAún no hay calificaciones
- 1 s2.0 S1877056819302713 MainDocumento12 páginas1 s2.0 S1877056819302713 MainMarianoAún no hay calificaciones
- Fracturas de TobilloDocumento23 páginasFracturas de TobilloGregorio VillarrealAún no hay calificaciones
- Varus Knee Classification and CorrectionDocumento8 páginasVarus Knee Classification and CorrectionPraharshaAún no hay calificaciones
- Overview of Tibial Fractures in Adults - UpToDateDocumento21 páginasOverview of Tibial Fractures in Adults - UpToDateJose LuceroAún no hay calificaciones
- Complications of The Surgical Treatment of Fractures of The Tibial Plateau Prevalence, Causes, and ManagementDocumento15 páginasComplications of The Surgical Treatment of Fractures of The Tibial Plateau Prevalence, Causes, and ManagementraynaldidjohariofcAún no hay calificaciones
- Tibial Plateau FractureDocumento7 páginasTibial Plateau FractureHerryanto AgustriadiAún no hay calificaciones
- 2019 Article 755Documento11 páginas2019 Article 755yayu latifahAún no hay calificaciones
- Foot and Ankle Injuries of The AthleteDocumento24 páginasFoot and Ankle Injuries of The AthleteSurgicalgownAún no hay calificaciones
- Microsoft Word - THR Preprint - Thr+PreprintDocumento2 páginasMicrosoft Word - THR Preprint - Thr+PreprintNuno GueiralAún no hay calificaciones
- Coding Arthroscopic Knee ProceduresDocumento13 páginasCoding Arthroscopic Knee Proceduresjeevan moreAún no hay calificaciones
- Quadrimalleolar Fractures of The Ankle: Think 360°-A Step-By-Step Guide On Evaluation and FixationDocumento3 páginasQuadrimalleolar Fractures of The Ankle: Think 360°-A Step-By-Step Guide On Evaluation and FixationFRANCISCOAún no hay calificaciones
- Bleazey-2012-Recon of Complex Oc Lesions of The Talus With Cylindrical Sponge Allograft and Particulate Juvenile Cartilage GraftDocumento7 páginasBleazey-2012-Recon of Complex Oc Lesions of The Talus With Cylindrical Sponge Allograft and Particulate Juvenile Cartilage Graftapi-212907483Aún no hay calificaciones
- 10.1007@s00264 019 04344 8Documento12 páginas10.1007@s00264 019 04344 8DavidAún no hay calificaciones
- Total Ankle Arthroplasty - Why Does It Fail?Documento7 páginasTotal Ankle Arthroplasty - Why Does It Fail?drjorgewtorresAún no hay calificaciones
- Marcheggianimuccioli 2019Documento12 páginasMarcheggianimuccioli 2019Ghusun MadaniAún no hay calificaciones
- Early Nontraumatic Fracture..... 3-39Documento5 páginasEarly Nontraumatic Fracture..... 3-39HAKAN PARAún no hay calificaciones
- How To Avoid Varus Stem in THRDocumento6 páginasHow To Avoid Varus Stem in THRPoliceAún no hay calificaciones
- 1 s2.0 S088354032100629X Main PDFDocumento7 páginas1 s2.0 S088354032100629X Main PDFBhudhavudhikrai WinAún no hay calificaciones
- Srugical Treatment of Complex Meniscus Tear and DiseaseDocumento11 páginasSrugical Treatment of Complex Meniscus Tear and DiseaseEfrain RodrigoAún no hay calificaciones
- Morbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesDocumento8 páginasMorbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesAthenaeum Scientific PublishersAún no hay calificaciones
- 1 s2.0 S1067251621001769 MainDocumento6 páginas1 s2.0 S1067251621001769 MainMervin AcostaAún no hay calificaciones
- jkhs-21-202 Ko enDocumento9 páginasjkhs-21-202 Ko enlaurenAún no hay calificaciones
- Abjs 6 105Documento7 páginasAbjs 6 105林良駿Aún no hay calificaciones
- Achot 2014 3 177 196 PDFDocumento20 páginasAchot 2014 3 177 196 PDFfunmugAún no hay calificaciones
- 2020 Finite Element Analysis - Femur Malunion+knee OADocumento9 páginas2020 Finite Element Analysis - Femur Malunion+knee OAstudmmaAún no hay calificaciones
- Closing Wedge Osteotomy of The Tibia and The FemurDocumento12 páginasClosing Wedge Osteotomy of The Tibia and The Femuralyek92Aún no hay calificaciones
- 2021 Acetabular Wear in THADocumento9 páginas2021 Acetabular Wear in THAilanAún no hay calificaciones
- The Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsDocumento8 páginasThe Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsanujAún no hay calificaciones
- Minimally Invasive Distal Metatarsal Osteotomy in The Treatment of Primary MetatarsalgiaDocumento23 páginasMinimally Invasive Distal Metatarsal Osteotomy in The Treatment of Primary Metatarsalgiamandala22Aún no hay calificaciones
- Ligament Balancing Medial Stabilising TechniqueDocumento6 páginasLigament Balancing Medial Stabilising TechniqueMohan DesaiAún no hay calificaciones
- Artigo ClamshellDocumento15 páginasArtigo ClamshellbritocirurgiadamaoAún no hay calificaciones
- Zimmer Trabecular Metal Total Ankle Surgical TechniqueDocumento76 páginasZimmer Trabecular Metal Total Ankle Surgical TechniqueAnkira FindoroAún no hay calificaciones
- The Iliotibial Tract: Imaging, Anatomy, Injuries, and Other PathologyDocumento19 páginasThe Iliotibial Tract: Imaging, Anatomy, Injuries, and Other PathologyBeah Marie AlisosoAún no hay calificaciones
- Osteoarthritis and Osteoporosis 2Documento38 páginasOsteoarthritis and Osteoporosis 2tarikeopsAún no hay calificaciones
- Postoperative KneeDocumento15 páginasPostoperative Kneeradiology residentsAún no hay calificaciones
- Current Concepts in Open-Wedge High Tibial Osteotomy: Review ArticleDocumento11 páginasCurrent Concepts in Open-Wedge High Tibial Osteotomy: Review ArticleAhmed SalmanAún no hay calificaciones
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentDe EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiAún no hay calificaciones
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesDe EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychAún no hay calificaciones
- Short ImplantsDe EverandShort ImplantsBoyd J. TomasettiAún no hay calificaciones
- Flexor Tendon Repair, Rehabilitation, and Reconstruction: Preoperative AssessmentDocumento11 páginasFlexor Tendon Repair, Rehabilitation, and Reconstruction: Preoperative AssessmentAdRiaNa JuLIetH LoZaDa PaTiÑoAún no hay calificaciones
- Hip DislocationDocumento4 páginasHip DislocationcrunkestAún no hay calificaciones
- BNO72122 - v2 - 161956 Focal Spasticity Workbook - FINAL - PIDocumento51 páginasBNO72122 - v2 - 161956 Focal Spasticity Workbook - FINAL - PIAli Radhi MutarAún no hay calificaciones
- Dariel Fitzkee - Linking Ring Manipulation PDFDocumento32 páginasDariel Fitzkee - Linking Ring Manipulation PDFLuigi-igiuL100% (4)
- Chondromalacia Patellae. A Prospective Study: J Bone Joint Surg AmDocumento9 páginasChondromalacia Patellae. A Prospective Study: J Bone Joint Surg AmMladen DabićAún no hay calificaciones
- GFHDocumento34 páginasGFHaisa mutiaraAún no hay calificaciones
- Osg - Catalogue 2Documento4 páginasOsg - Catalogue 2Navodaya HealthcareAún no hay calificaciones
- Posture and Gait Analysis PresentationDocumento6 páginasPosture and Gait Analysis Presentationapi-550365743Aún no hay calificaciones
- Red Flag: MSK Services Pathway - Elbow PathologyDocumento7 páginasRed Flag: MSK Services Pathway - Elbow PathologyMuhammed ElgasimAún no hay calificaciones
- Test 1: Scapular Axillary Hair Test at The End of FlexionDocumento2 páginasTest 1: Scapular Axillary Hair Test at The End of FlexionFitria Dewi LestariAún no hay calificaciones
- Karate TermsDocumento5 páginasKarate TermsFlorinAún no hay calificaciones
- Lower Limb Positioning Peer MentoringDocumento92 páginasLower Limb Positioning Peer MentoringJae Em DiestroAún no hay calificaciones
- Biomechanics of Foot and AnkleDocumento34 páginasBiomechanics of Foot and AnkleKanwal KhanAún no hay calificaciones
- Significance of The Structure of Human SkeletonDocumento5 páginasSignificance of The Structure of Human SkeletonTodirenche LarisaAún no hay calificaciones
- Lower Back Pain Exercises - NHSDocumento4 páginasLower Back Pain Exercises - NHSthomas_matheusAún no hay calificaciones
- Quiz - Bones and MusclesDocumento1 páginaQuiz - Bones and MusclesSimranAún no hay calificaciones
- Latest BackIntelligence FWD Head Exercises PDFDocumento7 páginasLatest BackIntelligence FWD Head Exercises PDFmattiaAún no hay calificaciones
- G6 SCIENCE Q2 W1 MODULE 1 Skeletal SystemDocumento16 páginasG6 SCIENCE Q2 W1 MODULE 1 Skeletal SystemMichelle Kirsten DELA Fuente100% (1)
- Shoulder Exam - OSCE StationsDocumento2 páginasShoulder Exam - OSCE StationsEmiel AwadAún no hay calificaciones
- LP 2 PDFDocumento6 páginasLP 2 PDFapi-380355050Aún no hay calificaciones
- Bnap (New) 2020Documento1 páginaBnap (New) 2020Jomalyn punzalanAún no hay calificaciones
- The Calisthenics Skill Tree (Template) 1.6.1Documento48 páginasThe Calisthenics Skill Tree (Template) 1.6.1KinDawn97Aún no hay calificaciones
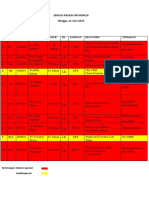
- Sensus Pasien Orthopedi Minggu, 21 JULI 2019: No Bed No - RM Nama Umur JK Jaminan Diagnosis TindakanDocumento3 páginasSensus Pasien Orthopedi Minggu, 21 JULI 2019: No Bed No - RM Nama Umur JK Jaminan Diagnosis TindakanWa JulianiAún no hay calificaciones
- 09 - Upper Limb 1 EditedDocumento52 páginas09 - Upper Limb 1 Editedshabnam sajidaAún no hay calificaciones
- Non Operative Fracture Management: Splint and CastDocumento78 páginasNon Operative Fracture Management: Splint and CastSaeda AhmedAún no hay calificaciones
- The Perfect Bicep Workout (2019)Documento4 páginasThe Perfect Bicep Workout (2019)itztonyAún no hay calificaciones