También podría gustarte
- 105643-Article Text-286411-1-10-20140722Documento2 páginas105643-Article Text-286411-1-10-20140722nurfadillahAún no hay calificaciones
- Communication With Patients, Families and Other ProfessionalsDocumento9 páginasCommunication With Patients, Families and Other ProfessionalsvabcunhaAún no hay calificaciones
- Chapter 4Documento27 páginasChapter 4rhassoun.228Aún no hay calificaciones
- SKenario Cros CultureDocumento24 páginasSKenario Cros CultureYusufi JieAún no hay calificaciones
- 2.B .Ndera CaseDocumento9 páginas2.B .Ndera CaseNsengimana Eric MaxigyAún no hay calificaciones
- Breaking Bad NewsDocumento6 páginasBreaking Bad NewsAdil IslamAún no hay calificaciones
- Harold Ellis Self AssessmentDocumento7 páginasHarold Ellis Self AssessmentIfeanyichukwu OgbonnayaAún no hay calificaciones
- Communication: Communication Is A Process of Sharing Information and Meaning, of Sending and Receiving MessagesDocumento5 páginasCommunication: Communication Is A Process of Sharing Information and Meaning, of Sending and Receiving MessagesNina OaipAún no hay calificaciones
- Supplementing Evidence-Based MedicineDocumento2 páginasSupplementing Evidence-Based MedicineSantiago HerreraAún no hay calificaciones
- Handling Aggressive Patients 1Documento3 páginasHandling Aggressive Patients 1Maria Lana Grace DiazAún no hay calificaciones
- 6 Dealling WTH Difficult PTDocumento9 páginas6 Dealling WTH Difficult PTprofarmah6150Aún no hay calificaciones
- Capitol Medical Center Colleges, Inc. College of Nursing NCM 105 - Lecture FinalsDocumento6 páginasCapitol Medical Center Colleges, Inc. College of Nursing NCM 105 - Lecture FinalsFaye Dianne Damian-BuenafeAún no hay calificaciones
- Breaking: Let Your Light Shine. Be The Source of Strenght and CourageDocumento21 páginasBreaking: Let Your Light Shine. Be The Source of Strenght and CourageYulia DamayantiAún no hay calificaciones
- Breaking Bad News: Ratna F. Soenarto R Besthadi Sukmono Dept. Anestesiologi & Terapi Intensif Fkui / RSCMDocumento30 páginasBreaking Bad News: Ratna F. Soenarto R Besthadi Sukmono Dept. Anestesiologi & Terapi Intensif Fkui / RSCMnikenseptiaAún no hay calificaciones
- The Art of History TakingDocumento54 páginasThe Art of History TakingChowdhury Shaheb MedicalwalaAún no hay calificaciones
- Nursing Diagnosis Keystone of Your Care PlanDocumento5 páginasNursing Diagnosis Keystone of Your Care Plandbryant010167% (3)
- 12 STEP Limit SettingDocumento2 páginas12 STEP Limit SettingOscar Esparza100% (1)
- DR Ruvaiz Haniffa: Dept. Family Medicine, Faculty of Medicine, University of Kelaniya 25 September 2006Documento17 páginasDR Ruvaiz Haniffa: Dept. Family Medicine, Faculty of Medicine, University of Kelaniya 25 September 2006Nipun M. DasanayakeAún no hay calificaciones
- Case Study of PhobiasDocumento8 páginasCase Study of PhobiasNsengimana Eric MaxigyAún no hay calificaciones
- Breaking Bad NewsDocumento25 páginasBreaking Bad Newslight tweenAún no hay calificaciones
- Medicine I 1.02 History TakingDocumento8 páginasMedicine I 1.02 History TakingrosamundraeAún no hay calificaciones
- They Can't Find Anything Wrong: 7 Keys to Understanding, Treating, and Healing Stress IllnessDe EverandThey Can't Find Anything Wrong: 7 Keys to Understanding, Treating, and Healing Stress IllnessCalificación: 3.5 de 5 estrellas3.5/5 (4)
- MKs Internal MedicineDocumento995 páginasMKs Internal Medicinejhqmpzg7sjAún no hay calificaciones
- Crisis Intervention: Psychiatric Nursing Nursing Care PlanDocumento13 páginasCrisis Intervention: Psychiatric Nursing Nursing Care PlanKatherine 'Chingboo' Leonico Laud100% (4)
- Beyond Breaking Bad NewsDocumento4 páginasBeyond Breaking Bad NewsNishtha KumarAún no hay calificaciones
- Active Listening SkillsDocumento58 páginasActive Listening SkillsNorjetalexis Maningo Cabrera100% (1)
- Health AssessmentDocumento4 páginasHealth Assessmentkatrina estanteAún no hay calificaciones
- Schizophrenia Fellowship Canterbury Newsletter Summer 2013Documento8 páginasSchizophrenia Fellowship Canterbury Newsletter Summer 2013Clare MouatAún no hay calificaciones
- Breaking Bad News 2014Documento75 páginasBreaking Bad News 2014lutvia100% (1)
- Active Listening SkillsDocumento6 páginasActive Listening SkillsJessaFamorAún no hay calificaciones
- Somatoform, Dissociative, Anxiety, Personality DisordersDocumento8 páginasSomatoform, Dissociative, Anxiety, Personality DisordersShamsa AfdalAún no hay calificaciones
- Communication Skills in MedicineDocumento5 páginasCommunication Skills in MedicineSGD blima semlimanamAún no hay calificaciones
- Seminar 3 1Documento16 páginasSeminar 3 1Maya BendelianiAún no hay calificaciones
- Survey The Scene: Quiday, Devorah Marie ADocumento1 páginaSurvey The Scene: Quiday, Devorah Marie ADevorah Marie QuidayAún no hay calificaciones
- Communication TechniquesDocumento10 páginasCommunication TechniquesNur Aleah MedtimbangAún no hay calificaciones
- React! Mental Health Poster - Response PlanDocumento1 páginaReact! Mental Health Poster - Response PlanEmmaAún no hay calificaciones
- The Search for Sanity: The Commonwealth and International LibraryDe EverandThe Search for Sanity: The Commonwealth and International LibraryCalificación: 4 de 5 estrellas4/5 (10)
- Plab 2 Notes Day 2Documento14 páginasPlab 2 Notes Day 2Beaulah0% (1)
- Talking With Your Older Patient A Clinician S HandbookDocumento8 páginasTalking With Your Older Patient A Clinician S HandbookDiana OliveiraAún no hay calificaciones
- Ethical Issues in The Management of Geriatric Cardiac PatientsDocumento3 páginasEthical Issues in The Management of Geriatric Cardiac PatientsOana Nicole StoicanAún no hay calificaciones
- Plab 2 Notes Day 2Documento14 páginasPlab 2 Notes Day 2Adnan Al JafaryAún no hay calificaciones
- Malingering?: Joseph H. Friedman, MD Joseph - Friedman@brown - EduDocumento6 páginasMalingering?: Joseph H. Friedman, MD Joseph - Friedman@brown - EduparahAún no hay calificaciones
- Oet Speaking 1-20Documento20 páginasOet Speaking 1-20Sharma KaushikAún no hay calificaciones
- Psikiatri EmergencyDocumento19 páginasPsikiatri Emergencyttotalitas23Aún no hay calificaciones
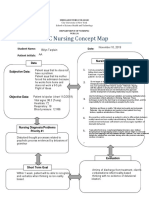
- Concept Map AADocumento2 páginasConcept Map AABillynTarplainAún no hay calificaciones
- Breaking Bad News HandoutDocumento8 páginasBreaking Bad News Handoutmedical chroniclesAún no hay calificaciones
- Mala NoticiaDocumento4 páginasMala NoticiaAleAún no hay calificaciones
- Dealing With Angry Patients and RelativesDocumento7 páginasDealing With Angry Patients and RelativesCalvin LooAún no hay calificaciones
- Broken Record TechniqueDocumento1 páginaBroken Record TechniquePratik VermaAún no hay calificaciones
- Neighbour - The Inner ConsultationDocumento5 páginasNeighbour - The Inner ConsultationjllayurAún no hay calificaciones
- Case Simulation 123 IjcgDocumento3 páginasCase Simulation 123 IjcgIrish Jane GalloAún no hay calificaciones
- Six-Word Lessons for Surviving a Devastating Diagnosis: 100 Lessons to Help You Navigate a Healthcare CrisisDe EverandSix-Word Lessons for Surviving a Devastating Diagnosis: 100 Lessons to Help You Navigate a Healthcare CrisisAún no hay calificaciones
- TOJ 18 0123 - 70mobleyDocumento4 páginasTOJ 18 0123 - 70mobleyRizka Uda'aAún no hay calificaciones
- Bmed137 PresentationDocumento30 páginasBmed137 Presentationapi-326400850Aún no hay calificaciones
- Process Recording, Suicide Assesment and Psyche-Med ConditionDocumento44 páginasProcess Recording, Suicide Assesment and Psyche-Med ConditionShy Dela PuertaAún no hay calificaciones
- Good Evidence and Positive Noticing: Beyond the Law of AttractionDe EverandGood Evidence and Positive Noticing: Beyond the Law of AttractionCalificación: 5 de 5 estrellas5/5 (2)
- An Insider's Guide To Getting The Best Out Of The Health SystemDe EverandAn Insider's Guide To Getting The Best Out Of The Health SystemAún no hay calificaciones
- First AidDocumento2 páginasFirst AidHannah DuyagAún no hay calificaciones
- Collecting Subjective DataDocumento18 páginasCollecting Subjective DataNadia SolohAún no hay calificaciones
- English Test 1 Xi SuggestionDocumento3 páginasEnglish Test 1 Xi SuggestionRabiah An Nikmah0% (1)
- End of BipolarityDocumento9 páginasEnd of Bipolarityekagrata100% (1)
- ChronologyDocumento4 páginasChronologyZoe Jenkins100% (1)
- Popular Culture BuhleDocumento19 páginasPopular Culture Buhlemongo_beti471Aún no hay calificaciones
- Lease ContractDocumento3 páginasLease ContractSometimes goodAún no hay calificaciones
- Fire ForceDocumento46 páginasFire Forcectenar2Aún no hay calificaciones
- Study Guide Vocab LWTW CH 11 18Documento5 páginasStudy Guide Vocab LWTW CH 11 18no bodyAún no hay calificaciones
- Jamnalal Bajaj Institute of Management: Telgi ScamDocumento14 páginasJamnalal Bajaj Institute of Management: Telgi ScamAnkita DesaiAún no hay calificaciones
- LEGASPI vs. Minister of FinanceDocumento2 páginasLEGASPI vs. Minister of FinanceAlex Gamboa100% (5)
- How Mexico Has Become The "Enemy" of America's RepublicansDocumento8 páginasHow Mexico Has Become The "Enemy" of America's RepublicansSUSANA SOSAAún no hay calificaciones
- Sara Lee Philippines Versus MacatlangDocumento3 páginasSara Lee Philippines Versus Macatlangganggingski50% (2)
- Ayala Investment and Development Corporation vs. CA, G.R. No. 118305Documento10 páginasAyala Investment and Development Corporation vs. CA, G.R. No. 118305graceAún no hay calificaciones
- Tataruka Usul-Adab HadorohDocumento23 páginasTataruka Usul-Adab HadorohWasta SupirAún no hay calificaciones
- Ciceron P. Altarejos, Petitioner, vs. Commission On Elections, Jose ALMIÑE and VERNON VERSOZA, Respondents. G, R. 163256 FactsDocumento4 páginasCiceron P. Altarejos, Petitioner, vs. Commission On Elections, Jose ALMIÑE and VERNON VERSOZA, Respondents. G, R. 163256 FactsFernan ParagasAún no hay calificaciones
- MACP SchemeDocumento15 páginasMACP SchemevkjajoriaAún no hay calificaciones
- Zamoras Vs Su Case DigestDocumento1 páginaZamoras Vs Su Case DigestChe Poblete CardenasAún no hay calificaciones
- Jess 406Documento8 páginasJess 406zippersandAún no hay calificaciones
- Bpop Plan - DanahaoDocumento3 páginasBpop Plan - DanahaoJessica CindyAún no hay calificaciones
- Racism and Rhetoric, From Ferguson To PalestineDocumento5 páginasRacism and Rhetoric, From Ferguson To PalestineThavam RatnaAún no hay calificaciones
- (Name of Proprietor, President or Authorized Representative), of Legal Age, - , Under Oath, Depose andDocumento1 página(Name of Proprietor, President or Authorized Representative), of Legal Age, - , Under Oath, Depose andRaymund100% (1)
- SVG ChattogramDocumento24 páginasSVG ChattogramMosharrofur Rahman ShahedAún no hay calificaciones
- 04.08.2022 S.no.116Documento2 páginas04.08.2022 S.no.116RUSHIK ZINZUVADIAAún no hay calificaciones
- The Lucis Trust - Satanism and The New World OrderDocumento5 páginasThe Lucis Trust - Satanism and The New World OrderPedro Pablo Idrovo Herrera100% (1)
- Grammar Questions (Set 4)Documento5 páginasGrammar Questions (Set 4)Snigdha TunuguntlaAún no hay calificaciones
- Private International Law NotesDocumento133 páginasPrivate International Law NotesKastriot B. BlakajAún no hay calificaciones
- History of Arnis EssayDocumento2 páginasHistory of Arnis EssayNatss VillanuevaAún no hay calificaciones
- Taller 3 de InglesDocumento4 páginasTaller 3 de InglesOMAR ARLEY CASTRO ROMEROAún no hay calificaciones
- In The Court of SHDocumento2 páginasIn The Court of SHBhalla & BhallaAún no hay calificaciones
- Diary EntryDocumento1 páginaDiary EntryAntonio EleuteriAún no hay calificaciones
- Pak Afghanistan Int RelationsDocumento4 páginasPak Afghanistan Int Relationstribalkhan100% (1)