También podría gustarte
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Compact Yet Robust: Chemistry AnalyzerDocumento4 páginasCompact Yet Robust: Chemistry AnalyzerThiago GalloAún no hay calificaciones
- Peter Attia Measuring Cardiovascular Disease Risk and The Importance of ApoBDocumento14 páginasPeter Attia Measuring Cardiovascular Disease Risk and The Importance of ApoBabhimanyu50% (2)
- UVA Family Medicine QbankDocumento32 páginasUVA Family Medicine QbankjamesmgangAún no hay calificaciones
- Nutrition Module 10Documento51 páginasNutrition Module 10SandeeAún no hay calificaciones
- Synthesis and Functions of CholesterolDocumento28 páginasSynthesis and Functions of CholesterolUbaid AhmedAún no hay calificaciones
- CLINICAL CHEMISTRY: ANALYTES AND SPECIMEN HANDLINGDocumento12 páginasCLINICAL CHEMISTRY: ANALYTES AND SPECIMEN HANDLINGAsherLamataoObeja0% (1)
- Lipoproteins in Diabetes Mellitus: Alicia J. Jenkins Peter P. Toth Timothy J. Lyons EditorsDocumento468 páginasLipoproteins in Diabetes Mellitus: Alicia J. Jenkins Peter P. Toth Timothy J. Lyons EditorsFELELAún no hay calificaciones
- The Influence of Silent Mutations On Pre-mRNA SplicingDocumento24 páginasThe Influence of Silent Mutations On Pre-mRNA SplicingAtikaWidyaSyariAún no hay calificaciones
- The Role of Renin Angiotensin Aldosteron System Genes in The Development of Hypertrophy Ini Hyperthrophic CardiomyopathyDocumento190 páginasThe Role of Renin Angiotensin Aldosteron System Genes in The Development of Hypertrophy Ini Hyperthrophic CardiomyopathyAtikaWidyaSyariAún no hay calificaciones
- Stevens-Johnson Syndrome Induced by Carbamazepine Treatment in A Patient Who Previously Had Carbamazepine Induced PruritusDocumento4 páginasStevens-Johnson Syndrome Induced by Carbamazepine Treatment in A Patient Who Previously Had Carbamazepine Induced PruritusAtikaWidyaSyariAún no hay calificaciones
- Top Three Pharmacogenomics and Personalized Medicine Applications at The Nexus of Renal Pathophysiology and Cardiovascular MedicineDocumento24 páginasTop Three Pharmacogenomics and Personalized Medicine Applications at The Nexus of Renal Pathophysiology and Cardiovascular MedicineAtikaWidyaSyariAún no hay calificaciones
- Association Between The HLA-B 15-02 Allele and Carbamazepine-Induced Stevens-Johnson Syndrome Toxic Epidermal Necrolysis in Han Individuals of Northeastern ChinaDocumento7 páginasAssociation Between The HLA-B 15-02 Allele and Carbamazepine-Induced Stevens-Johnson Syndrome Toxic Epidermal Necrolysis in Han Individuals of Northeastern ChinaAtikaWidyaSyariAún no hay calificaciones
- Silent Polymorphisms Can The TRNA Population Explain Changes in Protein PropertiesDocumento16 páginasSilent Polymorphisms Can The TRNA Population Explain Changes in Protein PropertiesAtikaWidyaSyariAún no hay calificaciones
- Silent Mutation Characterization of Its Potential As A Mechanism For Sterol 14demethylase Resistance in Cercospora Beticola Field Isolates From The United States 2157 7471 1000280Documento8 páginasSilent Mutation Characterization of Its Potential As A Mechanism For Sterol 14demethylase Resistance in Cercospora Beticola Field Isolates From The United States 2157 7471 1000280AtikaWidyaSyariAún no hay calificaciones
- Association Between HLA-B 1502 Allele and Carbamazepine-Induced Severe Cutaneous Adverse Reactions in Han People of Southern China MainlandDocumento3 páginasAssociation Between HLA-B 1502 Allele and Carbamazepine-Induced Severe Cutaneous Adverse Reactions in Han People of Southern China MainlandAtikaWidyaSyariAún no hay calificaciones
- Silent Mutations Make Some NoiseDocumento3 páginasSilent Mutations Make Some NoiseAtikaWidyaSyariAún no hay calificaciones
- Frozen ShoulderDocumento1 páginaFrozen ShoulderAtikaWidyaSyariAún no hay calificaciones
- Price of Silent MutationsDocumento12 páginasPrice of Silent MutationsAtikaWidyaSyariAún no hay calificaciones
- Benign Prostatic Hyperplasia and The Risk Of.12Documento8 páginasBenign Prostatic Hyperplasia and The Risk Of.12AtikaWidyaSyariAún no hay calificaciones
- Brakial Plexus InjuryDocumento1 páginaBrakial Plexus InjuryAtikaWidyaSyariAún no hay calificaciones
- Epidural HemorageDocumento1 páginaEpidural HemorageAtikaWidyaSyariAún no hay calificaciones
- Carpal Tunnel SindromDocumento1 páginaCarpal Tunnel SindromAtikaWidyaSyariAún no hay calificaciones
- Low Back PainDocumento1 páginaLow Back PainAtikaWidyaSyariAún no hay calificaciones
- Hernia UmbilicalDocumento1 páginaHernia UmbilicalAtikaWidyaSyariAún no hay calificaciones
- Typhoid Fever PDFDocumento4 páginasTyphoid Fever PDFAtikaWidyaSyariAún no hay calificaciones
- Hipo Album inDocumento1 páginaHipo Album inAtikaWidyaSyariAún no hay calificaciones
- Kaur PDFDocumento13 páginasKaur PDFAtikaWidyaSyariAún no hay calificaciones
- Hisprung DiseaseDocumento1 páginaHisprung DiseaseAtikaWidyaSyariAún no hay calificaciones
- Tgs Indvdu Drg. DendyDocumento1 páginaTgs Indvdu Drg. DendyAtikaWidyaSyariAún no hay calificaciones
- Yerba Mate Review: Effects on Weight, Lipids, Glycemia & MoreDocumento13 páginasYerba Mate Review: Effects on Weight, Lipids, Glycemia & MoreJuanManuelCabarcosAún no hay calificaciones
- Ho Lester OlllDocumento6 páginasHo Lester OlllVlad VladAún no hay calificaciones
- Coconut Oil: A Review: Agro Food Industry Hi Tech January 2014Documento5 páginasCoconut Oil: A Review: Agro Food Industry Hi Tech January 2014April mae heyresAún no hay calificaciones
- Antihyperglycemic and Antihyperlipidemic Potentials of Psidium GuajavaDocumento2 páginasAntihyperglycemic and Antihyperlipidemic Potentials of Psidium GuajavaThomy PrastomoAún no hay calificaciones
- Rizki Ayu Dwi Setianingrum G2B014005: Repository - Unimus.ac - IdDocumento15 páginasRizki Ayu Dwi Setianingrum G2B014005: Repository - Unimus.ac - IdToni Salvatio SidaurukAún no hay calificaciones
- Lipids & Treatment of DyslipidaemiaDocumento24 páginasLipids & Treatment of Dyslipidaemianizarsale7Aún no hay calificaciones
- Exp InstructionsDocumento10 páginasExp InstructionsLiterally NoOneAún no hay calificaciones
- Diabetes and HerbsDocumento132 páginasDiabetes and HerbsAjmal KhanAún no hay calificaciones
- Equipment Applications Microlab 200Documento29 páginasEquipment Applications Microlab 200Shan AhmadAún no hay calificaciones
- Dislipidemia Lancet Durrington PDFDocumento15 páginasDislipidemia Lancet Durrington PDFAlphaJulissa JuarezAún no hay calificaciones
- A Bornstein, MD, FACC Assistant Professor of Public Health Weill Cornell Medical CollegeDocumento50 páginasA Bornstein, MD, FACC Assistant Professor of Public Health Weill Cornell Medical CollegeSyed ImranAún no hay calificaciones
- VELARDE-Pharmacology Notes Unit B-Cardiovascular System-2019Documento19 páginasVELARDE-Pharmacology Notes Unit B-Cardiovascular System-2019j blAún no hay calificaciones
- Neutriderm Moisturising LotionDocumento13 páginasNeutriderm Moisturising LotionUASPharmaceuticalsAún no hay calificaciones
- Ped102 Module 1Documento20 páginasPed102 Module 1Lorida MelodyAún no hay calificaciones
- Prasugrel and RosuvastatinDocumento7 páginasPrasugrel and RosuvastatinMohammad Shahbaz AlamAún no hay calificaciones
- West Fairview P.EDocumento23 páginasWest Fairview P.EMau OlivaresAún no hay calificaciones
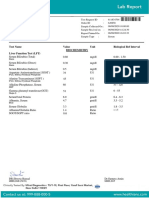
- Test Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Documento7 páginasTest Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Himanshu GarkhelAún no hay calificaciones
- LabreportnewDocumento14 páginasLabreportnewRajesh SharmaAún no hay calificaciones
- 159 CT10240Documento2 páginas159 CT10240thureinwinnAún no hay calificaciones
- Healthy Lifestyle Guidelines Mapeh JDocumento41 páginasHealthy Lifestyle Guidelines Mapeh JRos A LindaAún no hay calificaciones
- The BROAD Study: A Randomised Controlled TrialDocumento10 páginasThe BROAD Study: A Randomised Controlled Trialmoogle masterAún no hay calificaciones
- Written Report Coronary Heart DiseaseDocumento5 páginasWritten Report Coronary Heart DiseaseJade WushuAún no hay calificaciones
- Acute High Intensity Interval Cycling Improves MetabolismDocumento10 páginasAcute High Intensity Interval Cycling Improves Metabolismsilvio da costa guerreiroAún no hay calificaciones