También podría gustarte
- Create Consent Form (39 charactersDocumento3 páginasCreate Consent Form (39 charactersJan Diel100% (2)
- Anterior Cruciate Ligament-Injury & ManagementDocumento101 páginasAnterior Cruciate Ligament-Injury & ManagementYusuf Brilliant100% (1)
- Arthritis astrology signs and planetsDocumento5 páginasArthritis astrology signs and planetsJatinder SandhuAún no hay calificaciones
- Overcoming Low Self-Esteem Extract PDFDocumento40 páginasOvercoming Low Self-Esteem Extract PDFMarketing Research0% (1)
- Maths On The Move' - Effectiveness of Physically-Active Lessons For Learning Maths and Increasing Physical Activity in Primary School StudentsDocumento22 páginasMaths On The Move' - Effectiveness of Physically-Active Lessons For Learning Maths and Increasing Physical Activity in Primary School Studentsiisu-cmse libraryAún no hay calificaciones
- Lima Modular Revision Hip SystemDocumento32 páginasLima Modular Revision Hip SystemjsdanielinAún no hay calificaciones
- Breast LumpDocumento2 páginasBreast Lumplentini@maltanet.netAún no hay calificaciones
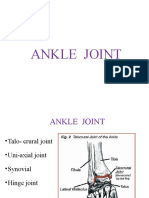
- ANKLE JOINT: THE HINGE OF THE FOOTDocumento29 páginasANKLE JOINT: THE HINGE OF THE FOOTRamakrishnanAún no hay calificaciones
- Clubfoot Pathophysiology and Ponseti TreatmentDocumento24 páginasClubfoot Pathophysiology and Ponseti TreatmentwildanmalikAún no hay calificaciones
- Foot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDDocumento55 páginasFoot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDrizwan.mughal1997Aún no hay calificaciones
- Management of Avn HipDocumento13 páginasManagement of Avn Hipterencedsza100% (1)
- SUTGMultiLocJ9981A PDFDocumento60 páginasSUTGMultiLocJ9981A PDFLouis MiuAún no hay calificaciones
- Pricippriles of Intramedullary NailingDocumento57 páginasPricippriles of Intramedullary NailingAbdallah OmerAún no hay calificaciones
- Ankle ComplexDocumento95 páginasAnkle ComplexMangala Prema MohanarangamAún no hay calificaciones
- Tendon Transfers For Radial Nerve PalsyDocumento62 páginasTendon Transfers For Radial Nerve Palsyavinashrao39Aún no hay calificaciones
- GTS Surgical TechniqueDocumento22 páginasGTS Surgical TechniqueMaurinho MnhAún no hay calificaciones
- External Fixator 110222141011 Phpapp01 131027142629 Phpapp01Documento65 páginasExternal Fixator 110222141011 Phpapp01 131027142629 Phpapp01manjunathaAún no hay calificaciones
- I. X-Ray Image: Hindfoot Fractures By: Jeremy Tan and Sarah HillDocumento8 páginasI. X-Ray Image: Hindfoot Fractures By: Jeremy Tan and Sarah HillSheril MarekAún no hay calificaciones
- Ligamentous Injuries About The Ankle and Subtalar Joints: Hans Zwipp, MD, PHD, Stefan Rammelt, MD, Rene Grass, MDDocumento35 páginasLigamentous Injuries About The Ankle and Subtalar Joints: Hans Zwipp, MD, PHD, Stefan Rammelt, MD, Rene Grass, MDAnonymous kdBDppigEAún no hay calificaciones
- A AaaaaaaDocumento6 páginasA AaaaaaaAnonymous d9Bzr1Aún no hay calificaciones
- Radial Head FractureDocumento40 páginasRadial Head FractureammarAún no hay calificaciones
- Fractures of The Humeral ShaftDocumento25 páginasFractures of The Humeral ShaftMuhammad IqbalAún no hay calificaciones
- Ankle Fractures: A Literature Review of Current Treatment MethodsDocumento13 páginasAnkle Fractures: A Literature Review of Current Treatment Methodsadrian1989Aún no hay calificaciones
- Back and Spine Anatomy GuideDocumento7 páginasBack and Spine Anatomy GuideCarmela Beatriz Suelan100% (1)
- Ankle Anatomy and Blood Supply of TalusDocumento66 páginasAnkle Anatomy and Blood Supply of TalusShashank29 LakkalaAún no hay calificaciones
- The Ankle Joint: Articulating BonesDocumento5 páginasThe Ankle Joint: Articulating BonesJoe SpencerAún no hay calificaciones
- Articular Fractures: PrinciplesDocumento24 páginasArticular Fractures: Principlestom kurniawanAún no hay calificaciones
- SHOULDER INSTABILITY ManagDocumento18 páginasSHOULDER INSTABILITY ManagFarhan JustisiaAún no hay calificaciones
- Missed Monteggia FXDocumento16 páginasMissed Monteggia FXEric RothAún no hay calificaciones
- Screws and Plates: Fixation Mechanisms ExplainedDocumento38 páginasScrews and Plates: Fixation Mechanisms ExplainedWasim R. IssaAún no hay calificaciones
- Any PDFDocumento252 páginasAny PDFRaja VeerappanAún no hay calificaciones
- Radiography of the Hip: Recognizing Disease PatternsDocumento16 páginasRadiography of the Hip: Recognizing Disease PatternsVivi Evita DewiAún no hay calificaciones
- Galeazzi-Fracture 6Documento14 páginasGaleazzi-Fracture 6MIGUEL ANGEL MEJIA FERNANDEZAún no hay calificaciones
- Acetabular and Hip FractureDocumento133 páginasAcetabular and Hip FractureJuanita HenryAún no hay calificaciones
- The Intramedullary Nail Is Commonly Used For LongDocumento4 páginasThe Intramedullary Nail Is Commonly Used For LongUhuebor DavidAún no hay calificaciones
- Wound Care Dressings and Their Uses: Carolyn Watts MSN, RN, CWON Vanderbilt University Medical Center Nashville, TNDocumento34 páginasWound Care Dressings and Their Uses: Carolyn Watts MSN, RN, CWON Vanderbilt University Medical Center Nashville, TNSuciAún no hay calificaciones
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDocumento8 páginasCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanAún no hay calificaciones
- Trochanteric #Documento20 páginasTrochanteric #Prakash AyyaduraiAún no hay calificaciones
- Arm:Leg Fracture PDFDocumento11 páginasArm:Leg Fracture PDFHannaAún no hay calificaciones
- Avascular Necrosis of The Fibular SesamoidDocumento7 páginasAvascular Necrosis of The Fibular SesamoidAlex Yvan Escobedo HinostrozaAún no hay calificaciones
- Clavo para ClaviculaDocumento12 páginasClavo para ClaviculaMartinLydenAún no hay calificaciones
- Gamma NailDocumento49 páginasGamma NailMihaela HerghelegiuAún no hay calificaciones
- Introduction of MSK ImagingDocumento63 páginasIntroduction of MSK ImagingyeabsraAún no hay calificaciones
- Interface Pressure Between Socket - Using TekscanDocumento207 páginasInterface Pressure Between Socket - Using TekscanSérgio SilvaAún no hay calificaciones
- Basinga Idys C ZPDocumento26 páginasBasinga Idys C ZPruiduartAún no hay calificaciones
- Z Effect & Reverse Z Effect in PFNDocumento7 páginasZ Effect & Reverse Z Effect in PFNNandan SurAún no hay calificaciones
- Fractures of Distal Radius: An Overview: Family PracticeDocumento8 páginasFractures of Distal Radius: An Overview: Family Practicesuci triana putriAún no hay calificaciones
- Damage Control In Multitrauma and OrthopaedicsDocumento37 páginasDamage Control In Multitrauma and OrthopaedicsroroAún no hay calificaciones
- Retrograde Tibia Intramedullary Nailing in Tibiotalocalcaneal ArthrodesisDocumento14 páginasRetrograde Tibia Intramedullary Nailing in Tibiotalocalcaneal ArthrodesisAthenaeum Scientific PublishersAún no hay calificaciones
- Polyaxial Locking System: Numelock IIDocumento24 páginasPolyaxial Locking System: Numelock IIpecheniqAún no hay calificaciones
- Srugical Treatment of Complex Meniscus Tear and DiseaseDocumento11 páginasSrugical Treatment of Complex Meniscus Tear and DiseaseEfrain RodrigoAún no hay calificaciones
- Anatomy of Vertebral ColumnDocumento59 páginasAnatomy of Vertebral ColumnRivan DwiutomoAún no hay calificaciones
- Large Fragment Locking Compression Plate (LCP) : Technique GuideDocumento23 páginasLarge Fragment Locking Compression Plate (LCP) : Technique GuideLouis MiuAún no hay calificaciones
- The Lower LimbDocumento37 páginasThe Lower LimbFoday H KalokohAún no hay calificaciones
- Early Total Care To Early Appropriate Care What.2Documento8 páginasEarly Total Care To Early Appropriate Care What.2ChrisAún no hay calificaciones
- 12 - Rehabilitation After Fractures of - 2018 - Clinical Orthopaedic Rehabilitat PDFDocumento7 páginas12 - Rehabilitation After Fractures of - 2018 - Clinical Orthopaedic Rehabilitat PDFTolo CantallopsAún no hay calificaciones
- Facet Joint Pain-Advances in Patient Selection and TreatmentDocumento16 páginasFacet Joint Pain-Advances in Patient Selection and TreatmentthiagoAún no hay calificaciones
- Shoulder ComplexDocumento72 páginasShoulder Complexchadalawada harika100% (1)
- Gamma3 Trochanteric Nail 180 TécCirurgDocumento48 páginasGamma3 Trochanteric Nail 180 TécCirurgPetru GanganAún no hay calificaciones
- Shoulder Arthroscopy Patient Education Packet RayappaDocumento5 páginasShoulder Arthroscopy Patient Education Packet Rayappaapi-549337910Aún no hay calificaciones
- 05 Fractures of The Upper Extremity Part 2 - Dr. TanDocumento75 páginas05 Fractures of The Upper Extremity Part 2 - Dr. TanMonique BorresAún no hay calificaciones
- Archs of The Foot - May 023Documento33 páginasArchs of The Foot - May 023mrizvi334Aún no hay calificaciones
- Mosaicplasty 1030208g UsDocumento12 páginasMosaicplasty 1030208g UsAnil SoodAún no hay calificaciones
- Journeyii CR 00344v1 UsDocumento40 páginasJourneyii CR 00344v1 UsSufyanAún no hay calificaciones
- Jude's Quadriceps Plasty For Stiff KneeDocumento6 páginasJude's Quadriceps Plasty For Stiff KneeRaviAún no hay calificaciones
- Sarmiento - 2011Documento422 páginasSarmiento - 2011jmhinos4833Aún no hay calificaciones
- SHS.201.Lec-16 Joints of NeckDocumento82 páginasSHS.201.Lec-16 Joints of NeckHumaira ShahidAún no hay calificaciones
- G Yepes 1966Documento9 páginasG Yepes 1966Yusuf BrilliantAún no hay calificaciones
- Management of Peritonitis in Critically Ill PatientDocumento29 páginasManagement of Peritonitis in Critically Ill PatientYusuf BrilliantAún no hay calificaciones
- Window Anatomy PDFDocumento7 páginasWindow Anatomy PDFYusuf BrilliantAún no hay calificaciones
- Leptospira As An Emerging PathogenDocumento12 páginasLeptospira As An Emerging PathogenYusuf BrilliantAún no hay calificaciones
- Staph KeratinDocumento9 páginasStaph KeratinYusuf BrilliantAún no hay calificaciones
- Blood Supply of BrainDocumento12 páginasBlood Supply of BrainSharon Rose Genita Medez100% (1)
- Understanding ACL injuries: Causes, symptoms, diagnosis and treatment optionsDocumento23 páginasUnderstanding ACL injuries: Causes, symptoms, diagnosis and treatment optionsYusuf BrilliantAún no hay calificaciones
- Management of IV Fluids and Electrolyte Balance Slides PDFDocumento29 páginasManagement of IV Fluids and Electrolyte Balance Slides PDFYusuf BrilliantAún no hay calificaciones
- How To Read A Head CT: DR Mohamed El Safwany. MDDocumento60 páginasHow To Read A Head CT: DR Mohamed El Safwany. MDYusuf BrilliantAún no hay calificaciones
- Behavioural Anchored Rating ScalesDocumento1 páginaBehavioural Anchored Rating ScalesYusuf BrilliantAún no hay calificaciones
- Development of The Central Nervous SystemDocumento39 páginasDevelopment of The Central Nervous SystemRyan SaganAún no hay calificaciones
- Be Careful With This Fraudster Network Malaysian InvestmentDocumento14 páginasBe Careful With This Fraudster Network Malaysian InvestmentYusuf BrilliantAún no hay calificaciones
- A Rare Cause of Endocarditis: Streptococcus PyogenesDocumento3 páginasA Rare Cause of Endocarditis: Streptococcus PyogenesYusuf BrilliantAún no hay calificaciones
- Leptospira As An Emerging PathogenDocumento12 páginasLeptospira As An Emerging PathogenYusuf BrilliantAún no hay calificaciones
- Measles Virus PathogenesisDocumento12 páginasMeasles Virus PathogenesisYusuf BrilliantAún no hay calificaciones
- Measles Virus PathogenesisDocumento12 páginasMeasles Virus PathogenesisYusuf BrilliantAún no hay calificaciones
- Measles Virus PathogenesisDocumento12 páginasMeasles Virus PathogenesisYusuf BrilliantAún no hay calificaciones
- Slide PosterDocumento11 páginasSlide PosterYusuf BrilliantAún no hay calificaciones
- Super HumanDocumento1 páginaSuper HumanYusuf BrilliantAún no hay calificaciones
- Diagnosis HipoglikemiaDocumento4 páginasDiagnosis HipoglikemiaYusuf BrilliantAún no hay calificaciones
- Drag RaceDocumento1 páginaDrag RaceYusuf BrilliantAún no hay calificaciones
- File PetingDocumento1 páginaFile PetingYusuf BrilliantAún no hay calificaciones
- Crottt Uuuh AaaahhDocumento1 páginaCrottt Uuuh AaaahhYusuf BrilliantAún no hay calificaciones
- Gagal Jantung 2013Documento83 páginasGagal Jantung 2013Yusuf BrilliantAún no hay calificaciones
- Diagnosis HipoglikemiaDocumento4 páginasDiagnosis HipoglikemiaYusuf BrilliantAún no hay calificaciones
- Daftar PenyakitDocumento46 páginasDaftar PenyakitNindya RimaliviaAún no hay calificaciones
- ABSTRAKS STUDI ,,,SEKSUAL - AUSTRALIA - EditDocumento2 páginasABSTRAKS STUDI ,,,SEKSUAL - AUSTRALIA - EditYusuf BrilliantAún no hay calificaciones
- New Issues in Hypertension Blood Pressure (Juli 2005)Documento47 páginasNew Issues in Hypertension Blood Pressure (Juli 2005)Yusuf BrilliantAún no hay calificaciones
- Elderly Care IndiaDocumento3 páginasElderly Care IndiakasurvarAún no hay calificaciones
- Clinical Case in Contact Lenses, 1e - 2001Documento205 páginasClinical Case in Contact Lenses, 1e - 2001Miguel PalaciosAún no hay calificaciones
- Pharmacoeconomics - Part IIIDocumento29 páginasPharmacoeconomics - Part IIISima JabbariAún no hay calificaciones
- Chapter 1Documento6 páginasChapter 1Hema Priya AdityanAún no hay calificaciones
- List of Empanelled Hospitals/Diagnostic Centres, and Cghs RatesDocumento53 páginasList of Empanelled Hospitals/Diagnostic Centres, and Cghs RatesArputAún no hay calificaciones
- Candida Albicans and IridologyDocumento8 páginasCandida Albicans and IridologyFRANCISCO JAVIER GALEANOAún no hay calificaciones
- 2nd Brochure PDFDocumento2 páginas2nd Brochure PDFhappy855Aún no hay calificaciones
- Concept Map Draft ExampleDocumento2 páginasConcept Map Draft ExamplemeliAún no hay calificaciones
- Prolanis Information and Time Conformity Influence Prolanis UtilizationDocumento8 páginasProlanis Information and Time Conformity Influence Prolanis UtilizationFicka HanafiAún no hay calificaciones
- Aur VedaDocumento4 páginasAur VedaLalit MishraAún no hay calificaciones
- Autologous Transfusion Strategies to Reduce Allogeneic Blood UseDocumento31 páginasAutologous Transfusion Strategies to Reduce Allogeneic Blood Usethalida24100% (1)
- HaritakiDocumento3 páginasHaritakirathan15Aún no hay calificaciones
- Gastroenterología y Hepatología: Scientific LettersDocumento2 páginasGastroenterología y Hepatología: Scientific LettersAswin ArinataAún no hay calificaciones
- Contact AllergyDocumento39 páginasContact AllergylintangAún no hay calificaciones
- CaseDocumento31 páginasCaseErnes PutraAún no hay calificaciones
- Migraine Hemicrania and Its Homeopathic Permanent Cure - DR Bashir Mahmud ElliasDocumento6 páginasMigraine Hemicrania and Its Homeopathic Permanent Cure - DR Bashir Mahmud ElliasBashir Mahmud ElliasAún no hay calificaciones
- Standards OF Psychiatric Nursing PracticeDocumento15 páginasStandards OF Psychiatric Nursing Practicesameeram83Aún no hay calificaciones
- IM Injuction: Definition of Intramuscular InjectionDocumento8 páginasIM Injuction: Definition of Intramuscular InjectiondhanasundariAún no hay calificaciones
- Anderson2008 Levofloxasin A ReviewDocumento31 páginasAnderson2008 Levofloxasin A ReviewFazdrah AssyuaraAún no hay calificaciones
- Prevalence of thyroid dysfunctionDocumento32 páginasPrevalence of thyroid dysfunctiondalip kumarAún no hay calificaciones
- CLASS 1 - Image - Roles Revised June 260Documento48 páginasCLASS 1 - Image - Roles Revised June 260Marie-Lynne L'orAún no hay calificaciones
- Fall Risk Care Plan NHS PDFDocumento2 páginasFall Risk Care Plan NHS PDFBelayetAún no hay calificaciones
- Grief Work BlatnerDocumento7 páginasGrief Work Blatnerbunnie02100% (1)
- Beximco Pharma FinalDocumento14 páginasBeximco Pharma FinalAli Asgor Raton67% (3)