También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2102)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- High Yield Surgery Compatible Version PDFDocumento77 páginasHigh Yield Surgery Compatible Version PDFDuke71% (7)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- MCAT Hormones and EnzymesDocumento2 páginasMCAT Hormones and EnzymesDevie Saha100% (3)
- Leeson Plan MemmlersDocumento34 páginasLeeson Plan Memmlersj01scott100% (1)
- Bariatric SurgeryDocumento252 páginasBariatric SurgeryEdward-Dan Buzoianu100% (2)
- 2023 - Ent Vivas FrcsDocumento331 páginas2023 - Ent Vivas FrcsPG ORL PUCEAún no hay calificaciones
- Learn The Brachial Plexus in Five Minutes or LessDocumento21 páginasLearn The Brachial Plexus in Five Minutes or LesskavithaAún no hay calificaciones
- Enhancing Surgical PerformanceDocumento86 páginasEnhancing Surgical Performanceeiad-mahmoud100% (1)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Mattox Maneuver - Statpearls - Ncbi BookshelfDocumento4 páginasMattox Maneuver - Statpearls - Ncbi Bookshelfeiad-mahmoudAún no hay calificaciones
- Energy - Rule 2 The Law of Conservation EDocumento1 páginaEnergy - Rule 2 The Law of Conservation Eeiad-mahmoudAún no hay calificaciones
- International English Language Testing System - WikipediaDocumento82 páginasInternational English Language Testing System - Wikipediaeiad-mahmoudAún no hay calificaciones
- AKI New GuidelineDocumento39 páginasAKI New GuidelineMohd RafiAún no hay calificaciones
- Energy - Rule 2 The Law of Conservation EDocumento1 páginaEnergy - Rule 2 The Law of Conservation Eeiad-mahmoudAún no hay calificaciones
- Energy Forms CarriersDocumento4 páginasEnergy Forms Carrierseiad-mahmoudAún no hay calificaciones
- An Algorithm For Abdominal Wall ReconstructionDocumento16 páginasAn Algorithm For Abdominal Wall Reconstructioneiad-mahmoudAún no hay calificaciones
- EnergySRP Forms MatchingDocumento2 páginasEnergySRP Forms Matchingeiad-mahmoudAún no hay calificaciones
- كيف تستخدم حروف الجر الإنجليزية - Kaplan BlogDocumento3 páginasكيف تستخدم حروف الجر الإنجليزية - Kaplan Blogeiad-mahmoudAún no hay calificaciones
- Purdue OWL - Irregular VerbsDocumento2 páginasPurdue OWL - Irregular Verbseiad-mahmoudAún no hay calificaciones
- EnergyDocumento1 páginaEnergyeiad-mahmoudAún no hay calificaciones
- Malignant Tumors ThyroidDocumento1 páginaMalignant Tumors Thyroideiad-mahmoudAún no hay calificaciones
- Anorectal Abscess Fistula PDFDocumento1 páginaAnorectal Abscess Fistula PDFeiad-mahmoudAún no hay calificaciones
- Chronic Atrophic Rhinitis - WikipediaDocumento2 páginasChronic Atrophic Rhinitis - Wikipediaeiad-mahmoudAún no hay calificaciones
- Complications of Thyroid Surgery - Practice Essentials, Overview, BleedingDocumento7 páginasComplications of Thyroid Surgery - Practice Essentials, Overview, Bleedingeiad-mahmoudAún no hay calificaciones
- Anatomy - Abdomen - Foramen of Winslow (Omental - Epiploic) - Statpearls - Ncbi Bookshelf PDFDocumento3 páginasAnatomy - Abdomen - Foramen of Winslow (Omental - Epiploic) - Statpearls - Ncbi Bookshelf PDFeiad-mahmoudAún no hay calificaciones
- Cymbalta (Duloxetine HCL) Patient Information - Side Effects and Drug Images at RxlistDocumento7 páginasCymbalta (Duloxetine HCL) Patient Information - Side Effects and Drug Images at Rxlisteiad-mahmoudAún no hay calificaciones
- Serotonin-Norepinephrine Reuptake Inhibitor - WikipediaDocumento6 páginasSerotonin-Norepinephrine Reuptake Inhibitor - Wikipediaeiad-mahmoudAún no hay calificaciones
- Chronic Atrophic Rhinitis - WikipediaDocumento2 páginasChronic Atrophic Rhinitis - Wikipediaeiad-mahmoudAún no hay calificaciones
- Vocal Fold Paresis - WikipediaDocumento3 páginasVocal Fold Paresis - Wikipediaeiad-mahmoudAún no hay calificaciones
- CerebrolysinDocumento14 páginasCerebrolysineiad-mahmoudAún no hay calificaciones
- CerebrolysinDocumento1 páginaCerebrolysineiad-mahmoudAún no hay calificaciones
- World Directory of Medical Schools - WFME ProjectsDocumento4 páginasWorld Directory of Medical Schools - WFME Projectseiad-mahmoudAún no hay calificaciones
- ReferencesDocumento1 páginaReferenceseiad-mahmoudAún no hay calificaciones
- Medical Board of Australia - International Medical Graduates (IMGs)Documento4 páginasMedical Board of Australia - International Medical Graduates (IMGs)eiad-mahmoudAún no hay calificaciones
- Osteocytes - Bone Cells Classifications of Bones According To SizeDocumento17 páginasOsteocytes - Bone Cells Classifications of Bones According To SizeA CAún no hay calificaciones
- Suprarenal GlandDocumento13 páginasSuprarenal GlandAaa JjjjAún no hay calificaciones
- How Do Organisms Reproduce Class 10 NotesDocumento17 páginasHow Do Organisms Reproduce Class 10 Notesjanesh rAún no hay calificaciones
- Group 10: Peripheral Nervous System (PNS)Documento24 páginasGroup 10: Peripheral Nervous System (PNS)Tara DolotaAún no hay calificaciones
- Chapter 13 - The Peripheral Nervous System and Reflex ActivityDocumento53 páginasChapter 13 - The Peripheral Nervous System and Reflex Activityramadan100% (1)
- Biology 3rd Lab Report (Animal Cell)Documento4 páginasBiology 3rd Lab Report (Animal Cell)Johanna Haludilu67% (3)
- Scanning Election Microscopic Study of Human Red Blood Cell Abnoinormalities in Fluoride ToxicityDocumento16 páginasScanning Election Microscopic Study of Human Red Blood Cell Abnoinormalities in Fluoride Toxicityijsidonlineinfo100% (3)
- Complications of Bed RestDocumento51 páginasComplications of Bed Restsuderson100% (1)
- EnglishDocumento6 páginasEnglishPH 1 9 6 0 9 Dao Phuong NamAún no hay calificaciones
- Lesson 4 - Cell ModificationsDocumento18 páginasLesson 4 - Cell ModificationsArvin Jay LamberteAún no hay calificaciones
- Cancer Staging - National Cancer InstituteDocumento3 páginasCancer Staging - National Cancer InstituteJadecharm GlariadaAún no hay calificaciones
- PyelonephritisDocumento59 páginasPyelonephritisGheyl GabrielAún no hay calificaciones
- Necropsy Techniques: General Pathology (VPM 152) Jan 2008Documento5 páginasNecropsy Techniques: General Pathology (VPM 152) Jan 2008Naresh RaviAún no hay calificaciones
- A. Sound FoundationDocumento47 páginasA. Sound FoundationKashmira TadaAún no hay calificaciones
- Mechanisms of Autoimmunity: - Recent ConceptDocumento4 páginasMechanisms of Autoimmunity: - Recent ConceptAdhimas Rilo PambudiAún no hay calificaciones
- Preparati HistologijaDocumento23 páginasPreparati HistologijaMarija Spasic100% (2)
- 1 Gcse Aqa BiologyDocumento43 páginas1 Gcse Aqa Biologycharlotteamy10Aún no hay calificaciones
- Science 9 Quarter 1 Week 3 Sim 4Documento17 páginasScience 9 Quarter 1 Week 3 Sim 4Rodel CamposoAún no hay calificaciones
- Gen Bio 2 Summative Test Q4 Week 1 and 2Documento3 páginasGen Bio 2 Summative Test Q4 Week 1 and 2Daniel Angelo Esquejo ArangoAún no hay calificaciones
- Cavum Oris Dan Galndula SalivariusDocumento26 páginasCavum Oris Dan Galndula SalivariusAisyah FawAún no hay calificaciones
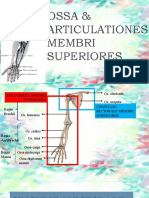
- Ossa & Articulationes 1Documento20 páginasOssa & Articulationes 1Wazna Rosyidatul AhsantiAún no hay calificaciones
- DR. Dr. Andhika Rachman - Basic Imunotherapy PDAIDocumento38 páginasDR. Dr. Andhika Rachman - Basic Imunotherapy PDAIsu wandyAún no hay calificaciones
- Excretory System of InvertebratesDocumento4 páginasExcretory System of InvertebratesHINA SHAHZADIAún no hay calificaciones
- Unicellular and Multicellular OrganisemsDocumento54 páginasUnicellular and Multicellular Organisemsmenaga ilangkovanAún no hay calificaciones
- Cell BiologyDocumento8 páginasCell BiologySharad DahalAún no hay calificaciones
- Final Physiology... Medical 2Documento12 páginasFinal Physiology... Medical 2Ishaq DerbashiAún no hay calificaciones