También podría gustarte
- Assessment of Patient Satisfaction in Public Hospitals in Cyprus A Descriptive StudyDocumento13 páginasAssessment of Patient Satisfaction in Public Hospitals in Cyprus A Descriptive StudyerwhuanAún no hay calificaciones
- HemorhoidDocumento60 páginasHemorhoidI Wayan MahardikaAún no hay calificaciones
- 1752 1947 8 453 PDFDocumento4 páginas1752 1947 8 453 PDFI Wayan MahardikaAún no hay calificaciones
- Plasmodium Knowledi PDFDocumento8 páginasPlasmodium Knowledi PDFI Wayan MahardikaAún no hay calificaciones
- 1752 1947 8 453 PDFDocumento4 páginas1752 1947 8 453 PDFI Wayan MahardikaAún no hay calificaciones
- Physiology of Bone Formation, Remodeling, and MetabolismDocumento30 páginasPhysiology of Bone Formation, Remodeling, and MetabolismDonny KurniawanAún no hay calificaciones
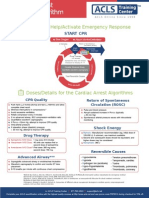
- Shout For Help/Activate Emergency Response: CPR StartDocumento2 páginasShout For Help/Activate Emergency Response: CPR StartdavpierAún no hay calificaciones
- Plasmodium Knowledi PDFDocumento8 páginasPlasmodium Knowledi PDFI Wayan MahardikaAún no hay calificaciones
- Physiology of Bone Formation, Remodeling, and MetabolismDocumento30 páginasPhysiology of Bone Formation, Remodeling, and MetabolismDonny KurniawanAún no hay calificaciones
- Kunci Jawaban Soal USGDocumento1 páginaKunci Jawaban Soal USGI Wayan MahardikaAún no hay calificaciones
- Review Pathophysiology and Recent Advances in The Management of Renal OsteodystrophyDocumento12 páginasReview Pathophysiology and Recent Advances in The Management of Renal OsteodystrophyI Wayan MahardikaAún no hay calificaciones
- Physiology of Bone Formation, Remodeling, and MetabolismDocumento30 páginasPhysiology of Bone Formation, Remodeling, and MetabolismDonny KurniawanAún no hay calificaciones
- Kunci Jawaban Soal USGDocumento1 páginaKunci Jawaban Soal USGI Wayan MahardikaAún no hay calificaciones
- Body Mass Index Table - To Calculate From Inches and PoundsDocumento1 páginaBody Mass Index Table - To Calculate From Inches and PoundsI Wayan MahardikaAún no hay calificaciones
- 0911 0189 BMI - Imperial PDFDocumento1 página0911 0189 BMI - Imperial PDFI Wayan MahardikaAún no hay calificaciones
- Hfa-Wfa 2-19 Girls en ExtendedDocumento1 páginaHfa-Wfa 2-19 Girls en ExtendedI Wayan MahardikaAún no hay calificaciones
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- PREM AlgorithmsDocumento20 páginasPREM AlgorithmsalexAún no hay calificaciones
- Broken Heart Syndrome: DiagnosticsDocumento25 páginasBroken Heart Syndrome: DiagnosticsOlga Goryacheva100% (1)
- 10.1007@s11604 019 00901 8Documento15 páginas10.1007@s11604 019 00901 8sayed hossein hashemiAún no hay calificaciones
- College Nursing Exam ReviewDocumento8 páginasCollege Nursing Exam ReviewKenneth NovenoAún no hay calificaciones
- ScccvyDocumento7 páginasScccvyDavy JonesAún no hay calificaciones
- Transcript 247 Pectasol C Modified Citrus Pectin and The Toxins It Removes With Dr. Isaac EliazDocumento16 páginasTranscript 247 Pectasol C Modified Citrus Pectin and The Toxins It Removes With Dr. Isaac EliazField90Aún no hay calificaciones
- Etiology of Eating DisorderDocumento5 páginasEtiology of Eating DisorderCecillia Primawaty100% (1)
- Muskan Agarwal ?Documento47 páginasMuskan Agarwal ?Ankit KumarAún no hay calificaciones
- Low Frequency Tens "Transcutaneos Electrical Nervestimulation"Documento72 páginasLow Frequency Tens "Transcutaneos Electrical Nervestimulation"Florian BeldimanAún no hay calificaciones
- Arthritis Fact SheetDocumento2 páginasArthritis Fact SheetClaire MachicaAún no hay calificaciones
- Vas 1Documento10 páginasVas 1Abdul Latiful KhabirAún no hay calificaciones
- Lifestyle DiseasesDocumento44 páginasLifestyle Diseaseskyro draxAún no hay calificaciones
- The Endocrine SystemDocumento14 páginasThe Endocrine SystemCrisanto Christopher Bidan Sanares100% (3)
- Management of ITP in ChildrenDocumento11 páginasManagement of ITP in ChildrenAndhika RahmawanAún no hay calificaciones
- Atom Electrosurgical SystemDocumento40 páginasAtom Electrosurgical SystemOgut AjaAún no hay calificaciones
- q2 Grade 9 Pe DLL Week 1Documento11 páginasq2 Grade 9 Pe DLL Week 1Airaa A. Baylan88% (8)
- Acute Appendicitis Made EasyDocumento8 páginasAcute Appendicitis Made EasyTakpire DrMadhukarAún no hay calificaciones
- History Taking and Physical ExaminationDocumento53 páginasHistory Taking and Physical ExaminationBoruuf If GammachuuAún no hay calificaciones
- Application of Functional Textiles in The Healthcare AreaDocumento1 páginaApplication of Functional Textiles in The Healthcare AreaSemana da Escola de Engenharia da Universidade do MinhoAún no hay calificaciones
- 50 Studies Every Anesthesiologist Shoud Know 2019Documento305 páginas50 Studies Every Anesthesiologist Shoud Know 2019pcut100% (2)
- Case ManagementDocumento4 páginasCase ManagementPraveena.R100% (1)
- Wardlaws Perspectives in Nutrition 9th Edition Byrd Bredbenner Test BankDocumento32 páginasWardlaws Perspectives in Nutrition 9th Edition Byrd Bredbenner Test Bankedricduyenuc1uw100% (19)
- Esophageal CancerDocumento3 páginasEsophageal CancerChanthorn SokAún no hay calificaciones
- Cardiovascular Physiology Applied To Critical Care and AnesthesiDocumento12 páginasCardiovascular Physiology Applied To Critical Care and AnesthesiLuis CortezAún no hay calificaciones
- Doctors Tell All-And It's Bad - Meghan O'Rourke - The AtlanticDocumento7 páginasDoctors Tell All-And It's Bad - Meghan O'Rourke - The AtlanticAlexAún no hay calificaciones
- Rehabilitation of Muscle Dysfunction in HemophiliaDocumento14 páginasRehabilitation of Muscle Dysfunction in HemophiliadavidcorzoAún no hay calificaciones
- Wellness Course Notes 2Documento1 páginaWellness Course Notes 2Eywon AbundoAún no hay calificaciones
- (IJCST-V9I3P10:Akshat Rustagi, Rudrangshu Tarafder, J. Rene BeulahDocumento7 páginas(IJCST-V9I3P10:Akshat Rustagi, Rudrangshu Tarafder, J. Rene BeulahEighthSenseGroupAún no hay calificaciones
- GallstonesDocumento17 páginasGallstonesع ب و دAún no hay calificaciones
- NCP Impaired Urinary EliminationDocumento2 páginasNCP Impaired Urinary EliminationTrixy Marie EcotAún no hay calificaciones