También podría gustarte
- Bisignano - Celsi LetterDocumento1 páginaBisignano - Celsi LetterThe GazetteAún no hay calificaciones
- Bond Shymansky - Press ReleaseDocumento1 páginaBond Shymansky - Press ReleaseThe GazetteAún no hay calificaciones
- Bond Shymansky University of Iowa ContractDocumento25 páginasBond Shymansky University of Iowa ContractThe GazetteAún no hay calificaciones
- 2018 09 20 IFA Independent Investigation Report (FINAL)Documento35 páginas2018 09 20 IFA Independent Investigation Report (FINAL)Kevin GlueckAún no hay calificaciones
- UIHC Coffee MapDocumento1 páginaUIHC Coffee MapThe GazetteAún no hay calificaciones
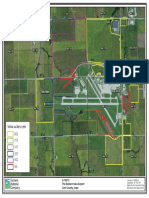
- Eastern Iowa Airport LandDocumento1 páginaEastern Iowa Airport LandThe GazetteAún no hay calificaciones
- Sierra Fox DocumentsDocumento51 páginasSierra Fox DocumentsThe Gazette100% (1)
- "Do You Know Fred Hubbell" AdDocumento1 página"Do You Know Fred Hubbell" AdThe GazetteAún no hay calificaciones
- Nov. 27 OCR LetterDocumento3 páginasNov. 27 OCR LetterThe GazetteAún no hay calificaciones
- VA LetterDocumento2 páginasVA LetterThe GazetteAún no hay calificaciones
- UI Road User Tax Study Final ReportDocumento315 páginasUI Road User Tax Study Final ReportThe GazetteAún no hay calificaciones
- WOTUS OrderDocumento2 páginasWOTUS OrderThe GazetteAún no hay calificaciones
- Middle Cedar Fact Sheet and MapDocumento2 páginasMiddle Cedar Fact Sheet and MapThe GazetteAún no hay calificaciones
- OCR Response To April 30 ReportDocumento6 páginasOCR Response To April 30 ReportThe GazetteAún no hay calificaciones
- WalzDocumento13 páginasWalzThe GazetteAún no hay calificaciones
- John Marshall Gazette 1980-09-17 Sound Inc LawyerDocumento1 páginaJohn Marshall Gazette 1980-09-17 Sound Inc LawyerThe GazetteAún no hay calificaciones
- NIR Alignment BoardDocumento1 páginaNIR Alignment BoardThe GazetteAún no hay calificaciones
- Top 3 Big Trees FINALDocumento8 páginasTop 3 Big Trees FINALThe GazetteAún no hay calificaciones
- Fy2017 University of Iowa NCAA ReportDocumento82 páginasFy2017 University of Iowa NCAA ReportThe GazetteAún no hay calificaciones
- Big Trees 7.1.2018Documento15 páginasBig Trees 7.1.2018The GazetteAún no hay calificaciones
- Ernst/Grassley Letter To Office of Inspector GeneralDocumento2 páginasErnst/Grassley Letter To Office of Inspector GeneralThe GazetteAún no hay calificaciones
- Big Trees of IowaDocumento8 páginasBig Trees of IowaThe GazetteAún no hay calificaciones
- IFOIC LetterDocumento3 páginasIFOIC LetterThe GazetteAún no hay calificaciones
- John Marshall Gazette 1983-12-18 Teleconnect Gets New LargerDocumento2 páginasJohn Marshall Gazette 1983-12-18 Teleconnect Gets New LargerThe GazetteAún no hay calificaciones
- Iowa Dem Tax Letter 2018Documento4 páginasIowa Dem Tax Letter 2018The GazetteAún no hay calificaciones
- Ford SettlementDocumento4 páginasFord SettlementThe GazetteAún no hay calificaciones
- Walz Energy Consent OrderDocumento10 páginasWalz Energy Consent OrderThe GazetteAún no hay calificaciones
- 2018-01-10 OCR Report Re Title IXDocumento32 páginas2018-01-10 OCR Report Re Title IXThe Gazette100% (1)
- John Marshall Gazette 1972-06-20 Objections To Phone Rate IncreaseDocumento1 páginaJohn Marshall Gazette 1972-06-20 Objections To Phone Rate IncreaseThe GazetteAún no hay calificaciones
- UnityPoint - St. Luke'sDocumento7 páginasUnityPoint - St. Luke'sThe GazetteAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- English For NursesDocumento3 páginasEnglish For Nursesnorasyidao50% (6)
- Caregiving Body TemperatureDocumento69 páginasCaregiving Body TemperatureDanny Line100% (1)
- TrueBeamBrochure RAD10119D September2013Documento16 páginasTrueBeamBrochure RAD10119D September2013DC ShekharAún no hay calificaciones
- AnalPleasureSlides PDFDocumento59 páginasAnalPleasureSlides PDFGorbatiuc Leonid67% (6)
- Sabiston Textbook of Surgery, 18th Ed. The Biological Basis of Modern Surgical PracticeDocumento5 páginasSabiston Textbook of Surgery, 18th Ed. The Biological Basis of Modern Surgical PracticeNunsio NallaAún no hay calificaciones
- Resident On Call PDFDocumento143 páginasResident On Call PDFMuhammad RezaAún no hay calificaciones
- Anaesthesia Syllabus BfuhsDocumento22 páginasAnaesthesia Syllabus BfuhsHarshit ChempallilAún no hay calificaciones
- Complication of FractureDocumento38 páginasComplication of FractureAshok BalwadaAún no hay calificaciones
- Total Thyroidectomy The Evolution ofDocumento8 páginasTotal Thyroidectomy The Evolution ofFasihul Lizan100% (1)
- The Medico-Legal Back An Illustrated Guide, 2004 PDFDocumento210 páginasThe Medico-Legal Back An Illustrated Guide, 2004 PDFvitaarfianaAún no hay calificaciones
- RxPinoy Medical Tourism Philippines Guidebook 2007Documento36 páginasRxPinoy Medical Tourism Philippines Guidebook 2007rxpinoy100% (3)
- Pricelist2023 USDDocumento366 páginasPricelist2023 USDSalwa NursyahidaAún no hay calificaciones
- Essay On SchoolDocumento7 páginasEssay On Schoolafibyoabyfffry100% (2)
- The Preterm Labor Index and Fetal Fibronectin For.24Documento6 páginasThe Preterm Labor Index and Fetal Fibronectin For.24bombonlrAún no hay calificaciones
- Breakthrough Health - Ted BroerDocumento228 páginasBreakthrough Health - Ted BroerJOHN DEEREAún no hay calificaciones
- Indian Public Health Standards (IPHS)Documento2 páginasIndian Public Health Standards (IPHS)Nikcy N M NicklavoseAún no hay calificaciones
- Medical prescription abbreviation guideDocumento10 páginasMedical prescription abbreviation guideFemi AlfarishiAún no hay calificaciones
- Algorithm For Cant Intubate Cant VentilateDocumento8 páginasAlgorithm For Cant Intubate Cant VentilateprashsubbuAún no hay calificaciones
- Medical Device Startup Blink Device Company Announces 510 (K) Clearance of TwitchView Quantitative Monitor For Neuromuscular Blockade and Hires VP of Sales and MarketingDocumento2 páginasMedical Device Startup Blink Device Company Announces 510 (K) Clearance of TwitchView Quantitative Monitor For Neuromuscular Blockade and Hires VP of Sales and MarketingPR.comAún no hay calificaciones
- Ectopic PregnancyDocumento1 páginaEctopic PregnancyBheru Lal50% (2)
- Anthony Filly CVDocumento5 páginasAnthony Filly CVapi-289727140Aún no hay calificaciones
- Zygoma Implant Procedure GuideDocumento63 páginasZygoma Implant Procedure GuideKristina Robles100% (2)
- Placental Abruption: Causes, Risks, and TreatmentDocumento30 páginasPlacental Abruption: Causes, Risks, and TreatmentNafisat AdepojuAún no hay calificaciones
- Burn Project ReferencesDocumento2 páginasBurn Project Referencesapi-279967709Aún no hay calificaciones
- USMLE Step 3 CCS StrategiesDocumento6 páginasUSMLE Step 3 CCS StrategiesDuncan Jackson100% (1)
- IEC-Atlas of Endoscopic UltrasoundDocumento12 páginasIEC-Atlas of Endoscopic UltrasoundDannyAún no hay calificaciones
- MRS FARZANA BEGUM'S LAB REPORTDocumento4 páginasMRS FARZANA BEGUM'S LAB REPORTGB BHaskaRAún no hay calificaciones
- Septal Bounce .15Documento1 páginaSeptal Bounce .15Wawaa Dochi NimoAún no hay calificaciones
- Heart SurgeonDocumento8 páginasHeart SurgeonayaanmalikyaseenAún no hay calificaciones